
Storm surge poles are visible across the Outer Banks. These sentinels warn of potential flooding from powerful cyclones. Warming oceans and sea level rise make such flooding more likely.
All posts in category Climate Crisis
Friday For Future — Sea Level Rise, Storm Surge Poles, More Intense Cyclones

Posted by robertscribbler on January 14, 2023
https://robertscribbler.wordpress.com/2023/01/14/friday-for-future-sea-level-rise-storm-surge-poles-more-intense-cyclones/
Big Waves off Ireland, UK as Series of Storms Gather in the North Atlantic
Significant wave heights are in the range of 25-30 feet off Ireland as a progression of storms focuses on both Ireland and the UK over the next five days.
Share this:
Posted by robertscribbler on January 7, 2023
https://robertscribbler.wordpress.com/2023/01/07/big-waves-off-ireland-uk-as-series-of-storms-gather-in-the-north-atlantic/
No COVID-19 Didn’t Stop the Climate Crisis, But It’s Interacting with it in a Bad Way
As we stand in the grips of one major global crisis, one whose first wave of mass casualties may finally be starting a merciful down-slope (on April 27, 2020), it’s important not to lose sight of the other, larger, one. Yes, I’m talking about the Climate Crisis. And as I mention it, I would be remiss to fail to note that one is not like the other. In particular, the climate crisis is much worse when measured over longer time scales and taken in total.
In an April 21 address ahead of Earth Day, U.N. Secretary-General António Guterres stated:
“Currently, all eyes are on the COVID-19 pandemic, the biggest test the world has faced since the Second World War. We must work together to save lives, ease suffering, lessen the shattering economic and social consequences, and bring the disease under control. But, at the same time, let us not lose focus on climate change. The social and economic devastation caused by climate disruption will be many times greater than the current pandemic.”
The reason is that the climate crisis is on a path of escalating damage and danger so long as we continue burning fossil fuels. One that does not relent if the carbon emission itself does not permanently abate. One that in the broader sense is capable of spinning off multiple sub-crises or harmfully amplifying and influencing others. Or in a sense that is in a micro-way more specific to the present pandemic, as we touched on early in this web-book, climate crisis can help to worsen and spread new infectious diseases.
COVID-19, Air Pollution, Deforestation, Warm Weather Illnesses, and Health Systems Impacted by the Climate Crisis
In the context of the present COVID-19 pandemic, the climate crisis, and its driver (fossil fuel based pollution), produces a number of harmful infectious illness interactions that are worth pointing out. Namely, the air pollution that drives the climate crisis can increase the death rate from COVID-19, the deforestation that also helps to drive the climate crisis can serve as a driver for the emergence of new coronavirus based illnesses like COVID-19, that COVID-19, like Ebola is a novel infectious illness from a typically warmer weather region, and that the climate crisis has deleterious impacts on the global health system that challenges our ability to manage such a wide-ranging pandemic outbreak. As we’ll glimpse below, COVID-19’s interaction with climate change denial and its related anti-science bent, has also been particularly harmful.
Second Hottest January through March on Record for 2020
A larger update for the climate crisis, however, takes in a couple of basic data points that show we are still on a very damaging and destructive climate pathway. One that the COVID-19 based economic slowdown and related temporary reductions of emissions by itself cannot halt (more on this later). A path we won’t effectively depart from unless we exit the COVID-19 pandemic by enabling a rapid transition to clean energy and a related follow-on effort to draw down excess atmospheric carbon.

First quarter of 2020 was the second hottest on record according to NASA GISS. Image source: NASA.
The first key climate crisis data point we’ll explore in this installment is provided by the climate experts at NASA GISS, headed by Dr Gavin Schmidt. And it comes in the form of a global surface temperature analysis for the first quarter of 2020. For, according to NASA, during the months of January through March of 2020 global surface temperatures averaged about 1.19 degrees Celsius above 20th Century baseline measures. This is about a 1.41 degree Celsius departure above 1880s averages. Quite a bit higher than the past five year baseline at 1.15 C hotter than 1880s averages and just 0.06 C below the record hot first quarter of 2016. It is also disturbingly close to the IPCC identified first climate threshold mark at 1.5 C. A threshold which we are probably still about a decade and a half away from breaching over a five year average time-frame along the present fossil fuel burning pathway. But it’s still not fun seeing us so close to it at present.
With such an opener, 2020 may not become a new record hot year. Somewhat less likely given no El Nino is expected, but possible. And if it does, it would spell more trouble. We’ll wait for confirmation on the 2020 temperature trend coming from NASA GISS and Dr Gavin Schmidt — who has dutifully provided publicly helpful annual temperature path projections during recent years. Regardless, 2020 will likely come uncomfortably close to another record hot year. And such continuing severe global heat is certainly within a well-established trend of longer-term heating.
Atmosphere Still Filling up with Carbon
Of course the primary driver of climate crisis is fossil fuel burning and related emissions of greenhouse gasses into the Earth’s atmosphere. Emissions that have temporarily slowed down — possibly by as much as 5-10 percent for 2020 according to this report by Carbon Brief — but have not halted. And emissions would have to slow down by a lot more and for a lot longer to start having a positive impact on the Earth’s climate system.
According to Glen Peters, research director at CICERO: “Even if there is a slight decrease in global fossil CO₂ emissions in 2020, the atmospheric concentration of CO₂ will continue to rise. The atmosphere is like a (leaky) bathtub, unless you turn the tap off, the bath will keep filling up with CO₂.” A statement of basic facts that climate change deniers who attack science are even now trying to confuse (see this scientist’s statement to clarify).
Not only are top voices at CICERO chiming in on the issue of climate crisis and a COVID-19 related temporary economic slow-down. But recently the World Meteorological Organization issued its own statement on the matter noting — the economic and industrial downturn as a result of the Coronavirus pandemic is not a substitute for concerted and coordinated climate action.
Climate Science Deniers Continue to Publicly Demonstrate a Dangerous Incompetence on COVID-19
We could give flight to reason and join in the ranks of science deniers who ignore and refute experts at places like CICERO and the World Meteorological Organization. Basically the same set of people who downplay or attack the advice of experts (like those at the World Health Organization) and ignore facts at our own and everyone else’s peril (but we won’t). We could listen to people like the current occupant of the White House (but we don’t). A known climate science denier who’s also spent months attacking public health experts and defunding key disease fighting groups while also peddling questionable COVID-19 treatments like hydroxychloroquine of unproved, potentially harmful, effectiveness. Who on Thursday, April 23rd appeared to publicly suggest injecting disinfectants (like Windex and Bleach) into our bodies as a valid way to fight COVID-19 infection (Do not do this! It can kill you!).
Trump later walked his ridiculous and dangerous statements back, while blaming his usual scape-goat — the free press — for his own brazen incompetence. But his most recent fact-free and literally dangerous circus show again put public health at risk with the potential to drive some of those who take his statements verbatim to inflict harm upon themselves. It also precipitated public health advisories from officials and the makers of Bleach and Windex advising people to, well, not take the President’s apparent advice. We could put ourselves at further risk by listening to his quackery-defending supporters, now lifting up a familiar gas-lighter chorus to try to tell us what we all saw happen didn’t, and related cohorts. But this form of self-harm follower-ship, or of even entertaining it, is proving to be a very, very bad idea. For the tendency here to deny the science on one threat — COVID-19, that those clinging to a certain political ideology are incapable of managing responsibly — is apparently related to their inability to perceive the larger threat of climate crisis.
CO2 Strikes Above 416 Parts Per Million During April of 2020
So instead we will just do the smart, rational thing and listen to the actual experts (I know many of us already do, but unfortunately and increasingly obviously some still do not) — world-class scientists who have spent their lives researching the Earth’s climate system. Scientists like Dr Michael E Mann, Dr Katherine Hayhoe, Dr Terry Hughes, Dr Stefan Rahmstorf, Dr Peter Gleick, Dr Gavin Schmidt, Dr Eric Rignot and so many more. And the atmospheric greenhouse gas indicators for the climate crisis that these scientists follow are still heading in the wrong direction. Still building up. Still providing more heat trapping capacity for the Earth’s atmosphere and larger climate system.

The seasonal carbon dioxide trend for the past two years as measured at the Mauna Loa Observatory shows continuing increases driven by fossil fuel burning. Image source: The Keeling Curve.
At this time, atmospheric CO2 is hitting above a 416 parts per million average on a weekly basis. This is well above anything seen in at least the last 2.6 to 5.3 million years and likely since the Middle Miocene 15-17 million years ago. According to the real experts at NOAA, this greenhouse gas is the primary driver of the present Earth System heating we now observe (see the Earth Systems Research Lab’s Greenhouse Gas Index Page).
So both heat and its big driver CO2 are still heading in the wrong direction. And, no, the fossil fuel burning tap into the tub didn’t stop running, it just turned down a bit. Hopefully permanently — but that will depend on what kind of economic stimulus we provide to help get us out of this crisis. Particularly for what kinds of energy systems we decide to stimulate to help get the global economy back up and running (clean energy to help stop the climate crisis and business as usual fossil fuel burning to keep making it worse) when the COVID-19 pandemic ultimately abates.
Up next: Social Distancing and Waiting Until It’s Safe Enough to Re-Open
Share this:

Posted by robertscribbler on April 27, 2020
https://robertscribbler.wordpress.com/2020/04/27/no-covid-19-didnt-stop-the-climate-crisis-but-its-interacting-with-it-in-a-bad-way/
It’s Everywhere Now — COVID-19 A Global Viral Wildfire
It moved like a fire.
First flickering in China during December.
There it evaded detection early-on. The Chinese government demurring to provide reports on the virus for crucial days. Then it grew and grew. Expanding to the point that it raged to terrifying size in China during January and February. Evoking a sudden, serious and locally effective lock-down even as the Chinese government coordinated with world health bodies on what had now become a large and deadly-serious threat to both national and global security.
COVID-19 Leaps China’s Fire Break
China and world health bodies built up a kind of infectious disease fire break meant to contain the new virus. By the end of February, China’s own initial case numbers had rocketed to just below 80,000. The largest novel infectious disease outbreak of its kind in at least three decades. But the viral fire wasn’t finished. In fact, it was just getting started.

Like wildfires, viruses can rage out of control once they escape containment — forcing large-scale mitigation to save lives. Unfortunately, this is exactly what happened in the case of COVID-19. Above image is of the climate crisis worsened Fort McMurray wildfire of 2016. Image source: Government of Alberta.
Like a climate crisis amplified blaze, the initial outbreak size was immense. It cast highly infectious sparks in all directions. It presented a much greater opportunity for infection spread than the first SARS outbreak in 2002-2003, than subsequent MERS outbreaks, or during the Ebola outbreak. Even in the best of circumstances, the viral fire had become so large that it would have been difficult to fight from mid-February onward.
Multiple Conflagrations During February and March
Tightly packed ships, travelers on airlines, persons in large gatherings became super spreaders of the new viral fire. South Korea, then Iran, then Italy saw large outbreaks in February through early March. But smaller numbers bearing viral fire were moving elsewhere. And if containment mostly succeeded after a hard fight in the areas that were diligent, and ready, and equipped and lucky, it failed in places where leaders were lackadaisical or too slow, or who brutishly suppressed inconvenient information and science, or who were overconfident and didn’t take the threat seriously, or who lacked or sabotaged response and containment capability, or who were just unlucky.
The viral fire was canny. It found weaknesses. It mercilessly exploited them. It spread rapidly through these weak points to other regions. On March 11, 2020, the World Health Organization declared COVID-19 to be a global pandemic. By the end of March worldwide cases had expanded to more than ten times China’s initial load — hitting just over 860,000 by the last day of March. The illness’s capacity to spread had expanded by an order of magnitude. Even more grim, the loss of souls was beginning to mount as well — with deaths from the virus rising to 43,000 by this time.
Running Toward the Flames — U.S. Outbreak Becomes Largest in the World
But despite its vicious pace of expansion, overconfidence still appeared to sway many right-wing heads of state, media personalities, and government leaders. Downplaying of the viral threat was still prevalent through mid-March and even as shut-downs began to take hold some were already calling it an over-reaction. Others showed an amazing insane propensity to run toward the viral fire or urge their followers to do the same. Trump and fellows on the right in the U.S. peddled the false hope of silver bullet treatments like chloroquine putting many people at increased risk of deadly health complications like cardiac arrest. Politicians like Florida Congressman Matt Gaetz, who wore a gas mask to mock a COVID-19 vote in Congress, and British Prime Minister Borris Johnson would show cavalier attitudes toward social distancing — later coming down with the infection. In the case of Johnson, his battle with COVID-19 would go critical — putting him in the emergency room for the fight of his life.

Visual of global distribution of COVID-19 cases on April 24, 2020. Note that U.S. case numbers are the highest of any nation. This is true for mortality numbers as well. Image source: Worldometers.
So overconfidence itself became one of the biggest weak points for the viral fire to exploit. For the United States, the overconfidence would prove crucial as a containment failure there allowed the viral fire to explode into the largest national outbreak anywhere. Presenting serious risks both to U.S. and global citizens. In March and April, a rapid U.S. spread would ultimately result in about a million cases in the U.S. alone (as of this writing, on April 23rd, the U.S. total is 850,000 with the growth ranging between 25,000 and 30,000 cases per day). About one in every four hundred U.S. citizens would become hosts to the viral wildfire before May. The toll in lives would be serious — approaching 60,000 by April’s end for the U.S. alone (more than 48,000 U.S. deaths on April 23rd with between 1,100 and 2,700 more deaths each day). This as governors like Georgia’s Brian Kemp unwisely sought to relax stay at home policies early against the advice of health experts as daily infection rates were still near peak levels. The failures of overconfidence and not listening to experts being a hard lesson to unlearn for many — particularly those on the political right. Overall, the United States’ outbreak would be the largest first wave event anywhere on the globe — surpassing China’s initial explosion by more than an order of magnitude.
Large Viral Fires Everywhere — Including Hot Brazil
The story was similar in Europe where states like the, at first lackadaisical under Borris Johnson, U.K. and a seemingly unlucky Spain and France would see massive outbreaks to add to Italy’s major event. Germany would experience its own major outbreak. But containment efforts for that state would prove more diligent and effective. Total cases in these five countries would roughly equal that of the U.S. by the end of April — adding almost another million (also at about 850,000 on April 23rd but growing at around 15,000 cases per day which is considerably slower than the U.S. growth rate).
Large outbreaks in Russia, Saudi Arabia, Turkey, and Brazil would further feed into the global conflagration as May approached. With these four countries hosting about 210,000 cases as of April 23rd, but growing at a rate of about 12,000 cases per day combined. Brazil’s own large outbreak of about 46,000 by April 23rd also carried with it a warning. Spokespersons on COVID-19 have often assumed that it, like the flu, maintained a seasonal nature in which infection spread more rapidly at cold times of year, but that hot times would prove protective. The virus’s response to temperature may well be more complex and nuanced. Repeatedly, experts have cautioned that COVID-19 cold weather prevalence assertions are somewhat dubious and unproven. Notably the virus emerged from tropical and subtropical environments. So hot weather may have a limited ability to curtail infection rates. And Brazil’s own large outbreak has occurred in a hot weather region during a hot time of year. Showing that the virus is capable of rapid spread during hot, summer-like conditions.

By April 23rd, global case numbers and deaths continued to increase on at a steep rate with little sign of abatement. More than 185 nations had seen COVID-19 cases and the likelihood of subsequent viral waves remained high. Image source: Worldometers.
Including all outbreaks, by mid-to-late April, the fire had taken in 213 countries, areas and territories. On April 23rd, about two million, seven hundred thousand people had been infected across the globe. The case rate was growing by about 80,000 each day (2.4 million per month). And of those confirmed with infection, about 190,000 or seven percent had died. A grim tally that continued to swell by 5,000 to 8,000 each day. Showing the world would likely see a quarter million lost from the virus by some time in early May.
More Waves Could Follow
COVID-19 had defied expectation both for its ability to spread and for its apparent lethality. A disease capable of super-spread that is at present apparently seventy times more deadly than the seasonal flu among detected cases (See John’s Hopkins data on case fatality for individual countries here). Something that given present data is potentially capable of producing a global impact that is the worst seen from an infectious illness outbreak since the deadly flu Pandemic of 1918-1919 if it breaks out more fully. This all just as the first wave of viral fire is passing over the globe. And until a cure or a very effective treatment is found, the virus now exists in a high enough global density to produce multiple subsequent waves of infection even if the first wave is abated (it presently is ongoing). A virus that appears to be capable of defying the conventional understanding of seasonality. And one that is extraordinarily transmissible and tricky to contain.
(UPDATED)
Up Next: No COVID-19 Didn’t Stop the Climate Crisis, But it’s Interacting with in in a Bad Way
Share this:

Posted by robertscribbler on April 23, 2020
https://robertscribbler.wordpress.com/2020/04/23/its-everywhere-now-covid-19-a-global-viral-wildfire/
The Trouble With Testing Part 1 — “No Responsibility at All”
“The White House is now home to an inattentive, conspiracy-minded president. We should not underestimate what that could mean.” — The Atlantic in a special report on U.S. pandemic preparedness during the July/August 2018 issue.
“Anybody that wants a test can get a test. That’s what the bottom line is… and the tests are all perfect, like the letter was perfect. The transcription was perfect, right?” — Donald Trump on March 6 as U.S. was suffering a major shortage of COVID-19 test kits.
“I take no responsibility at all.” — Donald Trump when asked if he felt any responsibility for the persistent lags in U.S. testing capability on March 13.
“President Trump continues to falsely state that everyone who needs a COVID-19 test can get one.” — In an NPR interview conducted on April 2.
“Two and a half months after the first reported coronavirus case in the US, America still doesn’t have the capacity that it needs to track all cases…” — Vox.
*****
The need for testing during a virus epidemic is directly related to the number of infected persons. If the outbreak is small, the need for testing is also proportionately smaller. And if the outbreak is large, then the need for testing is subsequently much larger.
Ironically, the more testing happens early on, the more cases are identified early on, the more contacts are traced and isolated early on, the more the virus is ultimately contained and the lower the follow-on need for tests. The inverse is also true. The less testing, identifying, and containing of pandemic illness early on, the more tests will later be needed.

A failure to test, trace and isolate in the U.S. early on resulted in a massive COVID-19 outbreak necessitating nationwide mitigation. 1 in 5 people tested in the U.S. are still showing up as positive as of April 20th — indicating that tests are generally still occurring only for high risk persons and not for the broader population. Image source: Our World in Data.
Because less testing, identification and containment means an illness like COVID-19 can expand undetected, exponentially, and with far less constraint. Each failure to respond to this nasty disease pushes us up the scale in the need for a still greater response in the form of testing, isolation, sanitation, and ultimately mitigation. And if leadership is incapable of providing that response in a continuous escalation, then we end up with an ever-expanding disaster. That’s what we face here in the U.S. Because here a national leadership under Trump that utterly lacks responsibility is showing its dramatic incapacity.
A Question of Responsibility
What is responsibility? At its root — response. In a disaster, swift, decisive, and effective response is what it takes to prevent an expanding and uncontainable cascade of harm, economic loss, and loss of life. Without leadership responsibility, a sense of duty to the persons under leadership’s charge and a willingness to answer to others, to positively absorb criticism, to act, to overcome barriers in order to make effective action possible, then crisis and disaster response itself will be set up to fail.
In the context of COVID-19, U.S. leadership failure by a corrupt and incompetent Trump Administration has weighed heavily in loss of life and well-being. Specifically, the Administration’s failure to take the responsibility necessary to provide the tests Americans need has been a critical aspect of this failure.
Test Development Timeline in a Global Context
Unlike South Korea which took swift action and outran global COVID-19 testing capability, the U.S. response under Trump in the form of deploying viable test kits, has lagged it.
On December 30 and 31 of 2019, China and WHO had identified pnemonia-like cases of a new illness. By January 10-12 of 2020, China released the new disease (later called SARS-CoV-2 for the virus or COVID-19 for the illness the virus causes) genome to the world. Within just a few days, German scientists, using SARS-CoV as a reference, had developed a test that could identify a unique portion of the SARS-CoV-2 virus’s DNA. On January 17, the World Health Organization (WHO) adopted the German-based test, published the guidelines for developing the test, and began working with private companies to rapidly produce those tests and distribute them. As other agencies developed new tests, WHO would also publicly provide the new formulas. For example, WHO published China’s test development formula one week later on January 24.
The importance of WHO action at this stage was threefold. First, it provided information on how to manufacture an effective test. In other words, any country could take the WHO-provided information and use it to mass produce its own tests. Like South Korea, they could then independently coordinate with medical industry to get the production chain rolling. Unlike South Korea, they no longer needed to independently develop one. A test formula was now publicly available. Second, the WHO began to manufacture test kits to send out to other nations who requested them. These manufactured kits provided physical samples of the published testing formula — making it easier for manufacturers in other countries to validate and reproduce. Third, WHO served as an agency that mass produced tests. This helped to provide tests to those who were unable to provide for themselves. By March 16, two months later, WHO alone had produced 1,500,000 tests and sent kits out to 120 countries.

The gene assay of SARS-CoV provided by Olfert Landt to the World Health Organization in January. This assay would result in an easily producible test that many nations would use to contain their COVID-19 outbreak. Image source: WHO.
Independently, the German firm that provided the first test protocol adopted by WHO was also shipping out tests to other countries. In mid-January, New Zealand, who decided the WHO-published test formula was good enough and the need for more immediate access to tests was greater than the need to independently produce one at home, ordered the Germany-developed kits. The kits were subsequently shipped. And New Zealand was provided with tests ahead of the outbreak that later occurred. In other words — they were prepared. Australia and a number of other countries made the same decision — also ordering their test kits from overseas. Olfert Landt’s firm, the German Agency that developed the first COVID-19 test protocol adopted by WHO, alone was shipping out 1,500,000 tests per week by late February of 2020.
U.S. — All Testing Eggs Slow-Walked into one Trump-Shrunken Basket
In the U.S., the Centers for Disease Control, a crucial public health protection organ, had long suffered budget cuts and diminishment under Trump. As noted before, each of Trump’s budgets had requested reduced funding for CDC and his attacks on the Affordable Care Act also degraded U.S. disease fighting capability. His removal of Obama’s Pandemic Task Force had cut off a federal limb that could have helped stop the virus in its tracks overseas, but if it did get out could have also coordinated infectious disease response at home and abroad, cut red tape, and sped the availability of materials such as test kits for the U.S. public.
Perhaps as equally pivotal, though, was Trump’s choice of director — Robert Redfield — to head CDC. Redfield, unlike many of Trump’s appointees, was certainly a professional with many years of experience in his field. One who spent 30 years researching HIV and for 20 years served in the U.S. Army Medical Corps. Redfield was, arguably though, far from a great choice to head the agency responsible for fighting disease in the U.S. He was embroiled in a controversy over an HIV vaccination trial in the 1990s in which he was accused of manipulating data. Redfield has also been criticized for allowing his strong religious beliefs to interfere with his medical views. Peter Lurie from the Center for Science in the Public Interest, a consumer advocacy group expressed this concern about Redfield’s appointment: “What one would get in Robert Redfield is a sloppy scientist with a long history of scientific misconduct and an extreme religious agenda.”
In choosing the controversial Redfield, Trump also passed over Anne Schuchat — a career public servant whose experience dealing with Anthrax in the U.S., Ebola in West Africa, and SARS in China made her an ideal choice for CDC head. In other words, an infectious disease expert with exactly the kind of experience to handle an illness like COVID-19. That’s what the people of the United States didn’t get from Trump. What we got was something that we’ve come to expect from a corrupt and incompetent Administration — at best a political appointee with professional credentials but also possessed of a questionable and often partisan-charged past, at worst the same but with no professional standing whatsoever.
As it happened, on the same day that WHO had published Olfert Landt’s test kit formula on its website, January 17, a sapped CDC in the U.S. announced that it had developed its own preliminary test for COVID-19. They’d decided to work on their own test. This decision was guided in part by regulation — and much of it for good reason. We didn’t want to open the door to fraudulent tests. But it was also a decision that occurred in the context of a global health emergency. And leadership from the top could have worked to ensure the protective needs of regulation were adhered to while still providing back-up options if the CDC-sponsored test kit development occurred too slowly or didn’t produce a usable test soon enough.
In other words, they could have cut red tape to enable medical industry in the U.S. to produce coordinate tests. Like South Korea, they could have called together industry heads and provided organization and guidance. Something a dedicated pandemic response team, had it been in place, could have helped to accomplish. Something a CDC head with novel pandemic chops like Anne Schuchat would have recognized the need for. CDC could have worked to validate those tests in conjunction with its own test. It could have used one of a number of WHO-validated formulas for these coordinate tests. It could have set up teams to work to validate multiple sets of tests to determine which ones were effective. It could have worked to set up contingency surge production if more tests were needed (as happened in South Korea and elsewhere).

The bio of Anne Schuchat — the kind of infectious disease expert that the U.S. is capable of fielding to head an effective pandemic response. The kind of expert the Trump Administration has repeatedly passed over in favor of less effective leaders. Image source: CDC.
Such a layered strategy did not develop at CDC under Redfield as head. At first, and for many weeks after, the decision by leadership was to support one testing regime and then to in a laissez faire way, ignore the fact that other agencies such as FDA ended up using existing regulation to defend it and to (unintentionally) stymie the independent development of effective tests in the U.S. In other words, through lack of response adequate to the threat of COVID-19, Trump’s CDC head put all their testing eggs into one basket.
Making Our Own Unluck
It all could have still worked out. The U.S. could have been lucky. The CDC test could have worked effectively. It could have arrived in time to help stop the virus. It could have arrived in enough numbers to meet the testing need. It could have been targeted to the regions that needed it most. Trump’s Redfield CDC hadn’t increased their likelihood of that success, though. They had greatly increased the opportunity for failure. And given that self-infliction of a worsened set of odds, things did not go well.
Development of the CDC test notably lagged behind the rest of the world. By January 21, the U.S. saw its first confirmed case of COVID-19. It was of a man who’d flown back from Wuhan, China and entered the U.S. on January 15. But it took another week — until January 28th for the CDC to provide its own test kit formula to WHO — 11 days later than Germany, four days later than China, and weeks after South Korea had developed an effective test protocol. Fully two weeks after the virus had arrived on U.S. shores.
It wasn’t until February 5 — fully 19 days after CDC’s first test protocol was announced — that a CDC under Trump had shipped 200 test kits to more than 100 public health labs across the U.S. These tests were enough to test 60,000 – 80,000 people if the kits proved effective. By the same time, WHO had shipped 250,000 tests that had already been validated. Globally, on February 5, confirmed cases had risen to above 28,000. In the U.S., 12 cases had been confirmed with cases springing up Washington State, Illinois, Wisconsin, California, Massachusetts, and Arizona. Given what we know about COVID-19, actual numbers were probably already much greater than these early confirmations indicated.
The virus had arrived on U.S. shores and CDC had scrambled to send out these test kits. But the test deployment would ultimately prove to be seriously problematic. The trouble with these U.S. tests ended up being four-fold. First, that they had not yet (by February 5) been validated and many would later prove useless. Second, there weren’t enough to meet demand. Third, many came too late. And fourth, test kit distribution was not targeted or weighted to the regions of highest need. Why the U.S. CDC response was so much slower and so poorly coordinated compared to those of other nations has not fully been explained. Nor has it been fully explained why many of the tests that CDC ultimately provided would fail. But this failure was arguably a major reason why COVID-19 would break out to such a great extent in the U.S. Why the U.S. would experience the worst first wave outbreak of this novel deadly illness. Because what ultimately happened was a serious failure to contain the illness once it reached our shores. To perform that detection, contacts tracing and isolation that was proving so useful in places like South Korea.
So by early February, CDC had shipped out about 200 test kits to public health labs across the country. Each kit contained enough material to test between 300 to 400 patients. But because kits were evenly distributed, places with much higher populations, places like public health labs in New York City which would later experience a devastating outbreak, only received enough testing material to test between 300-400 patients at that time. That’s 300-400 tests for a public health lab serving a city of 8.4 million souls.
According to a report from Kaiser:
The kits were distributed roughly equally to locales in all 50 states. That decision presaged weeks of chaos, in which the availability of COVID-19 tests seemed oddly out of sync with where testing was needed.
Another problem was that the test kits that were shipped out often proved faulty — lacking critical components that hobbled kits ability to produce results. So from February 5 to mid February — for about ten days or so — public health labs across the country were put in the position where they needed to validate CDC test kits. And, in most cases, the validation of a useful kit did not occur. By mid-February only about six public health labs had access to reliable tests. But the Trump-appointed CDC director Robert Redfield was at the time entrenched, defending those tests. He insisted that CDC had developed a “very accurate test.”

Global distribution of COVID-19 cases on February 20, 2020. Image source: World Health Organization.
At this point the official number of cases stood at 15. But we know that those numbers were growing unchecked. Mainly because the CDC test kits would prove inadequate. On February 24th, U.S. confirmed cases had jumped to 53 and health experts were saying that community spread was happening in the U.S. On the same day, The Association of Public Health Laboratories sent a plea letter to the FDA asking if states could develop their own testing protocols independent of the CDC. In a few days, FDA reversed its previous position of defending CDC tests as a national standard and allowed states to begin producing their own tests. By February 29, after 43 days, the CDC tests had only been used 472 times. An astonishingly small number compared to the 60,000 to 80,000 that the original test kits should have represented. The U.S. confirmed case total stood at 68. But hundreds more people had already been infected by the illness in the U.S. We just didn’t have much of a way to know who or where because the CDC-backed testing regime ended up being so abysmal.
March Explosion
In the race between testing to track the illness and COVID-19’s in-built imperative to grow beyond our control in the U.S., the virus was winning. It had gotten a big head start of about a month and a half.
By early March, as the number of tests in the U.S. was finally starting to expand, in large part due to rapid production of tests within states and independent of the Trump-hobbled CDC, U.S. confirmed case totals were rapidly shooting upwards. On March 7, confirmed U.S. cases had hit 435. Redfield on the same day noted about the CDC tests: “We found that, in some of the states, it didn’t work. We figured out why. I don’t consider that a fault. I consider that doing quality control. I consider that success.”

By the end of March the U.S. COVID-19 case total would be the largest in the world. This would necessitate a nationwide lockdown as containment failed risking hundreds of thousands of deaths. Image source: Worldometers.
In one more week, confirmed cases would multiply nearly sevenfold — hitting 2,770 by March 14. Tests were finally starting to work and be produced in larger numbers. But for the U.S., a new worrying statistic was starting to become evident — the number of positive cases per test was notably high. In total about 1 out of every 4-5 people receiving a test were testing positive. This was due to the fact that the primary location for U.S. testing was hospitals and emergency rooms. The U.S. did not have widespread dedicated test facilities like South Korea. So most people who got a test were already very ill. All of this was an indication that the U.S. barely understood even the tip of the COVID-19 iceberg that the country was slamming up against.
By March 21, the number of COVID-19 cases had again exploded — hitting 24,345 or nearly ten times their number from the prior week. States such as Washington, New York, and California were testing thousands of people per day now. And a disturbing understanding of the U.S. disease curve was starting to emerge. A model produced by the Imperial College in London projected that as many as 2.2 million people in the U.S. could die if the U.S. did not move strongly to mitigate the spread of the virus.
Moving To Mitigation as Virus Outruns Containment in a Big Way
Unlike testing, contacts tracing, and isolation, mitigation involves serious constraints on activity within the impacted regions. In effect it would mean lockdowns or stay at home orders for much of the nation. A kind of freeze placed on society and economies in order to reduce mass loss of life. We say reduce, because the mass casualty event for the U.S. had already gotten well out of the bag. Tens of thousands would already lose their lives as a result. The question now was between tens of thousands and hundreds of thousands or millions along with a smashed U.S. hospital system.
By March 31, U.S. cases had again exploded to nearly 190,000. Even more tragically, already more than 4,000 souls had been lost due to the virus. A Trump Administration that had promised to provide 27 million tests by that time had only seen the U.S. testing 1 million. And a good portion of these tests were provided not by the CDC or the federal government under Trump, they were provided by states who were forced to scramble to fill the yawning vacuum of a failed federal testing, contacts tracing and isolation response.

Most U.S. states now have more than 1,000 COVID-19 cases. Many now have more than 10,000 cases. The U.S. total will likely near 1 million by the end of April. This massive outbreak has forced large scale mitigation in which most states remain under stay at home orders. Image source: CDC.
Now states would have to step in again. This time to provide the mitigation necessary to prevent about 2.2 million deaths across the U.S., California’s Gavin Newsom issued a stay at home order on March 19, New York’s Governor, Andrew Cuomo, made a similar order just a day later on March 20th, Washington State’s order came on March 25th, Maryland’s own stay at home order began on March 30th. By the end of March, fully 42 states had issued a stay at home policy. A policy that would remain in place for many weeks to come. Containment had failed in a dramatic way. Testing still lagged well behind the need. People who wanted tests still couldn’t get them. And as U.S. COVID-19 case numbers climbed toward 1 million in April, testing would continue to lag the need for it in most places.
The result was a full-on move to mitigate COVID-19’s spread. But the failure to provide enough tests would still haunt the U.S. And a new issue with testing would emerge as debates on how to restart a hobbled U.S. economy in the presence of a widespread and terrible virus that had wafted its way into all corners of our nation would again emerge. Sadly, this debate would continue to include a tone of irrational defiance to advice provided by experts and to the larger threat posed by a deadly and as yet incurable illness from the Trump Administration and its political supporters.
(UPDATED)
Up next: It’s Everywhere Now — COVID-19 A Global Viral Wildfire
Share this:

Posted by robertscribbler on April 20, 2020
https://robertscribbler.wordpress.com/2020/04/20/the-trouble-with-testing-part-1-no-responsibility-at-all/
Effective Containment — How South Korea’s First Coronavirus Wave was Halted
“Testing on its own will not stop the spread of SARS-CoV-2. Testing is part of a strategy. The World Health Organization recommends a combination of measures: rapid diagnosis and immediate isolation of cases, rigorous tracking and precautionary self-isolation of close contacts.” — COVID-19 Epidemic in Switzerland.
“South Korea has emerged as a sign of hope and a model to emulate. The country of 50 million appears to have greatly slowed its epidemic … Behind its success so far has been the most expansive and well-organized testing program in the world…” — Science Magazine.
“We acted like an army.” — Lee Sang-won, an infectious diseases expert at the South Korea Centers for Disease Control in a statement to Reuters.
*****
If U.S. leadership, under Trump, failed to initially prepare for, recognize, respond to, and effectively communicate to the public on the issue of COVID-19, there was a whole new set of failures surrounding the issue of infectious disease containment. Specifically involving the federal provision of enough tests to the public and to various infectious disease and emergency response agencies to stop a rapidly mounting COVID-19 threat. This failure is a part of the larger response failure by Trump and his administration. In particular, this containment failure was so crucial that it deserves a separate mention (next chapter).
But before we dig into the Trump Administration’s specific failure to provide the tests needed to conduct a successful disease outbreak containment, to gain an accurate picture of the disease outbreak during mitigation, or to provide any hope for an effective reopening of the economy following any successful mitigation, it’s helpful to look at the response of a nation that did manage a successful containment of COVID-19’s first wave. For a rapid response by South Korea, primarily through mass production of tests and subsequent contacts tracing and isolation, squashed what could have been a much more substantial first wave outbreak and ultimately managed to greatly limit new daily cases.
Testing and Containment
Detection and identification of cases, testing which according to CDC is an essential tool for detecting infectious agents, isolation of confirmed cases, contacts tracing, and isolation of confirmed contacts. In a single sentence, this basically defines a strategy of novel infectious disease outbreak containment (based on CDC’s after action reports on SARS response and CDC’s FAQ on SARS).
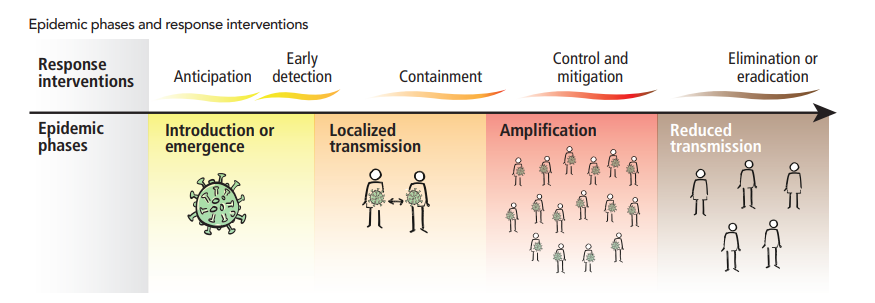
Epidemic phases and response interventions. Detection and containment are key responses. Availability of testing is critical for this phase of infectious disease response. Image source: World Health Organization.
It’s used when there’s a new illness outbreak that can’t be effectively treated or cured and when that illness represents a significant threat to life, well being, and a functioning society. In recent years, detection and containment was effective in halting both the first SARS outbreak in 2002 and 2003 and the major Ebola outbreak of 2013-2016. Containment is itself only as effective as the ability to positively identify — often best done through symptoms screening by astute healthcare professionals and testing — a majority of the active cases and to, through contacts tracing, identify each person contacted by the infected individual(s) and to isolate all those involved. If there are not enough tests to measure the number of people infected, if the information management resources do not exist to trace contacts, and if isolation of cases and contacts is not conducted in an effective manner, then containment is unlikely to succeed.
Containment should not be confused with mitigation. But it can be used alongside mitigation as part of a comprehensive strategy of disease response. Mitigation is a strategy to be used either in conjunction with containment of a large outbreak or when containment fails and a widespread outbreak begins to result in disease amplification and/or presents a threat to the effective functioning of healthcare infrastructure. Mitigation often involves social distancing — which is, in effect, the pre-emptive isolation of large sections of society to reduce contacts and to slow disease spread (we’ll talk more about mitigation in a later chapter).

Testing and positively identifying cases enables a second aspect of infectious disease containment — contact tracing. This practice can identify cases quickly and, in conjunction with isolation, prevent illness spread. Image source: CDC and CFCF.
Testing and containment is very important in its own right. It can stop an illness in its tracks. It can save thousands, tens of thousands, hundreds of thousands, or even millions of lives. In the present context of the COVID-19 pandemic, containment has succeeded where testing was widely available and when contacts tracing and isolation was conducted effectively. And in the worst outbreaks — such as in the U.S. — containment failed, in large part, due to lack of the capacity to conduct a large number of tests. This failure resulted in a greater outbreak which froze the economy and required large-scale mitigation to slow disease spread, maintain the ability of hospitals to function, and to reduce loss of life from millions to tens or hundreds of thousands.
South Korea — Learning Hard Lessons From MERS
The story of South Korea’s successful response to the first wave of COVID-19 pandemic begins back in 2015 when MERS was producing a global outbreak of new infectious illness. MERS was another novel disease similar to SARS in that it impacted the human respiratory system and resulted in high death rates. It emerged from yet another climatologically hot region — the Middle East. And MERS was still another novel coronavirus. One also with an ultimate origin in bats. However, MERS is thought to have a zoonosis due to harmful interactions between humans and camels. How MERS spread to camels from bats and then to humans remains somewhat unclear. Though it is thought that the consumption of poorly cooked camel meat is a likely vector for transfer of this new illness to human beings.
MERS was far more deadly than SARS — resulting in mortality in about 1/3 of those infected. Its geographic region of origin was the Middle East. And since the time when MERS was first identified in 2012, approximately 2519 individual infections have been reported on a global basis.

A map of MERS transmission and outbreaks. Human outbreak areas shown in red and blue. Note South Korean outbreak in upper right. Image source: WHO.
In 2015, South Korea had its own tough brush with MERS. At the time, a South Korean businessman became ill after a trip to three countries in the Middle East. He sought treatment at three South Korean health facilities before he was diagnosed with MERS and put under isolation. But his contacts over the interim period ultimately resulted in 184 MERS infections within South Korea and 38 deaths. During this period, South Korea conducted a major response effort to contain the horrifying illness. The prospect of a major epidemic sent alarm signals through the country, slowed its economy, and traumatized the public. In response, South Korea produced a, then major, testing, contacts tracing, and isolation response in order to contain the illness. In the end, over 17,000 people were quarantined in an effort that ultimately quashed the outbreak.
Alertness, Training, and an Early Response
Pneumonia-type illnesses appear to have ingrained themselves on the collective consciousness of South Koreans during recent years. The 2015 MERS outbreak was viewed by many as a wake-up call. But the earlier 2002-2003 SARS outbreak and a general understanding of the risks of new coronaviruses appear to have made their cultural mark as well.
Back in December of 2019, according to reports from Reuters, two dozen top infectious disease experts in South Korea conducted a tabletop exercise. The scenario was oddly prophetic — a family becomes infected with a pnemonia-like illness after a trip to China. In the scenario, the new illness could have been a new form of influenza or a coronavirus like MERS or SARS. The exercise left its mark. And the lessons learned from it would be crucial to South Korea’s rapid escalation.
Just one month later, South Korea was organizing a response to an actual coronavirus pandemic emerging from China. And they were about as ready as they would ever be due to a combination of preparation, concern, and apparent luck. On December 30 of 2019, China and WHO collected and analyzed samples of the novel coronavirus and then communicated first findings. And on January 4th, just five days later, South Korea’s infectious disease experts had access to a test methodology to positively identify COVID-19 cases. This was three days before China had genetically identified the new virus, it was five days before Chinese scientists uploaded a copy of SARS-CoV-2’s genome into an international repository. On January 9th they began lab testing for COVID-19.
They’d learned their lesson from MERS — quick response was absolutely necessary. And top experts still had the recent tabletop exercise fresh on their minds. But they still didn’t have a commercial, mass producible, test. The early testing methodology was slow. It could only manage a small number of cases at a time. As the disease began to rapidly expand in China, South Korean infectious disease experts feared they’d need something that was easily replicated on a mass scale.
On January 27th, South Korean infectious disease control personnel had detected just four cases of COVID-19 but they feared an epidemic. And their fears were rational. They’d experienced the explosive growth of MERS just a handful of years earlier and experts were starting to get hints that COVID-19 was a deceptive illness capable of both eluding detection and rapid expansion without widespread testing and isolation. On the same day, South Korean CDC officials summoned 20 heads of the nation’s medical industry. Their goal — turn South Korea’s lab test into a mass-produced, easy to use, diagnostic test. Just one week later, a diagnostic test produced by one of these companies was approved by South Korea’s CDC.
Lee Sang-won, infectious diseases expert at Korea’s Centers for Disease Control and Prevention, noted to Reuters — “We acted like an army.”
From Testing to Containment — South Korea’s Close Call
The problem with containing a disease like COVID-19 is that it is capable of seriously explosive spread. A single person infected with this illness who gets into a tightly packed setting with a large group or that moves rapidly from person-to-person can become what in disease parlance is known as a super-spreader. On February 18, just 11 days after South Korea had approved a commercially mass-producible test for COVID-19, a woman presenting symptoms who would represent South Korea’s 31st official case tested positive.
She was 61 years of age and, like many of us, she was a social person who delighted in her community. Part of her community was a rather large mega-church — the Shincheonji megachurch in Daegu, about 240 kilometers southeast of Seoul. When her contacts were traced it was found that she attended two services — one on February 9th and another on February 16th. At the time, she was already feeling slightly ill. In the church — 500 attendees would sit, tightly packed, through each 2 hour service.

Infection curve for South Korea shows a major spike in cases during late February and early March, then a rapid flattening that experts attribute to mass testing and isolation enabled by widely available tests for people with symptoms. Image Source: Worldometers.
From February 17 through 29, South Korea experienced an explosion of cases jumping from 31 to 3150. The vast majority of these new cases came from members of the Shincheonji megachurch. At this point, South Korea’s outbreak was the largest outside of mainland China. It was an outbreak that threatened to overwhelm the nation of 51 million people. South Korea’s 130 disease detectives were initially swamped by the Shincheonij-centered outbreak. More than 80 percent of patients with respiratory symptoms from this single outbreak were testing positive and the resources of South Korea’s traditional CDC response force was chiefly focused on this one cluster.
South Korea’s disease response teams were reeling. And without the earlier prep-work, they would have surely failed. As it was, South Korea just barely responded in time to prevent a much larger outbreak.
Responsible Governance Leads to Disease-Fighting Success
South Korea’s fast-tracked testing, contacts tracing and isolation system arrived in late February and rapidly expanded into March. This fast-tracking provided a key new disease response capability exactly when it was needed. By the end of February, just as its outbreak was ramping up, widespread road-side testing centers were opened. These centers were specifically set up to manage infected persons. Staff had personal protective equipment (PPE). They’d been trained in proper infection containment and sanitation protocols. And, in total, these centers were capable of testing thousands of people each day.

One of South Korea’s many drive-through testing centers. At this location, healthcare professionals wearing personal protective equipment (PPE) administer a COVID-19 test. Image source: Government of South Korea.
In addition, specialized government isolation centers were opened for persons infected with COVID-19 — adding an outside capacity that reduced stress to hospitals. People who tested positive were required to download an app on their phone that traced their past movements and contacts. These contacts were also required to download the phone app and to self-isolate. Violators of the self-isolation policy were fined a 2,500 dollar equivalent.
This larger second line of defense enabled South Korea’s health officials to capture cases and conduct larger isolation outside of the initial disease cluster. A massive public health defense infrastructure that effectively sprang up overnight in response to the illness. One that ultimately prevented larger spread, wider sickness, increased illness amplification and death, and a need for even larger resource allocation to fight the disease. A national resource that would prove crucial.
Looking at South Korea’s infection curve, you can see how effective South Korea’s policy of rapid response containment has been. The results speak for themselves. They should count themselves fortunate for the responsiveness and responsibility displayed by their national government and leading healthcare professionals. Their first wave infection curve would have been much worse without it. It could have looked like Italy, or worse, the United States.
(UPDATED — Clarification on South Korea research testing timeline vs China’s COVID-19 research and coordination with WHO.)
Up Next: The Trouble With Testing Part 1 — “No Responsibility at All”
Share this:

Posted by robertscribbler on April 14, 2020
https://robertscribbler.wordpress.com/2020/04/14/effective-containment-how-south-koreas-first-coronavirus-wave-was-halted/
Denial, Defunding, Downplaying — First COVID-19 Leadership Failures
“Decades of climate denial now appear to have paved the way for denial of Covid-19 by many on the right, according to experts on climate politics.” — Inside Climate News.
“The Democrats are politicizing the coronavirus… and this is their new hoax.” — Donald Trump.
“Just left the Administration briefing on Coronavirus. Bottom line: they aren’t taking this seriously enough. Notably, no request for ANY emergency funding, which is a big mistake. Local health systems need supplies, training, screening staff etc. And they need it now.” — Democratic Senator Chris Murphy
“Now, I want to tell you the truth about the coronavirus … Yeah, I’m dead right on this. The coronavirus is the common cold, folks.” — Rush Limbaugh
“It’s going to disappear. One day, it’s like a miracle, it will disappear.” — Donald Trump
“President Donald Trump has repeatedly undermined science-based policy as well as research that protects public health.” — the Environmental Data and Governance Initiative.
*****
In the ancient story, the prophet goes to confront the king. The prophet says — the Babylonians are coming, we must prepare, we must try to save our people. And the king says — I don’t believe it.
This is tragic. But it is also a dramatic failure of leadership and of a leader’s basic responsibility to protect those she or he serves. Because the point where disaster becomes inevitable is not when news of danger arrives. The point where disaster becomes inevitable, in the face of great danger, is when leadership sabotages itself and everything that relies on it. In the ancient story, the king’s denial is the death-knell for his civilization.
Science Denial As Climate Crisis Enabler
In America, we’ve done our best to remove ourselves from the curse of kings and their blind, cowardly, selfish pride that can hurt so many. But we are not immune to it. Far from it, with the political right now enamored with a novel authoritarianism, we are intensely vulnerable at this moment in history.
It is a vulnerability that we have seen play out again and again in the context of the climate crisis. With Inhoffe’s snowball in Congress, with Trump calling climate change a Chinese hoax during the 2016 election, with the thousands of false climate messages sent out by organizations like the Heartland Institute, with the ongoing attacks on climate scientists coming from platforms like Fox News, right-wing talk radio, and social media.
Even worse, we’ve seen this vulnerability of playing to unfettered and corrupt authority mutate into the climate crisis denial policies — huge subsidies for fossil fuels, erosion or removal of pollution controls, removing clean vehicle standards, hobbling or delaying clean energy systems like wind, solar, and EVs, smearing helpful policies like the Green New Deal, misinforming the public on the efficacy of climate solutions, attacking IPCC findings even while working to water down IPCC messaging, and attacking helpful global climate policies like Paris from every angle imaginable. In this way, a politics of denial becomes a platform both for harmful policy and for harmful behavior.
Anti-Science Denial Becomes Bludgeon
A new vulnerability emerged with COVID-19. A kind of right wing systemic weakness resulting from years of failure to listen to experts and to support the institutions that protect both those of us in the U.S. and people around the world from the ravages of a wave of emerging and re-emerging infectious illness. This vulnerability became visible as China was grappling with a monstrous outbreak during December of 2019 and January of 2020. It became still more apparent during February as COVID-19 threatened to go global, to strike deeply into the U.S. population as well. And by March the various failures of the Trump Administration would result in the U.S. suffering the worst of any nation from COVID-19’s global first wave.
But the failures of leadership that paved the way for COVID-19 to rapidly expand began months and years before. It began with anti-science and anti-public-health Trump-lackey-type Republicans taking control of the executive branch of the United States.
Sabotaging Global and US Pandemic Preparedness
The story of the Trump Administration’s erosion and removal of key U.S. and global protections in the time before the Coronavirus outbreak is extensive. We will touch on some of its highlights here. In short, the removal of protections was deep, it was systemic, and it arose from both the Administration and its supporters’ operating ideology which included actively eroding national and global institutions. It also centered on Trump himself — who seemed unwilling to listen to even his own followers, taking any seeming or perceived contradiction as an insult. Moreover, presented with facts, Trump has repeatedly seemed to consider them an affront to him personally. In this case, Trump and his loyal and unquestioning followers targeted the very institutions aimed at keeping our populations well.

2018 was the first fiscal year budget request by the Trump Administration. This graph by Kaiser is one indicator of how much Global Health was de-prioritized in the transition from Obama to Trump. Image source: Kaiser.
According to reports from Foreign Policy, in 2018 the Trump Administration fired the government’s entire pandemic response chain of command. This included the management infrastructure for pandemics within the White House. An observation that has been broadly validated.
In 2018, the Trump Administration also sought deep cuts in a program called the Global Health Security Agenda (GSHA). The program was aimed at shoring up other countries ability to detect pathogens. The GHSA aimed to set up a global early warning system for new outbreaks of infectious diseases.
In July of 2019, the Trump Administration told an infectious disease expert then in China whose job it was to assist Chinese disease response and to facilitate information sharing between the U.S. and China during a disease outbreak that her job was defunded. This caused her to leave her post. Overall, the Trump Administration dramatically reduced disease response capability in China. According to The Guardian, 11 CDC staffers charged with disease response were cut to three people, while 39 workers who supported them were reduced to 11 people.
In addition, Trump Admin budget requests have asked for a reduction in CDC funding by 15-20 percent for each of the past years. Coordinately, Trump’s attempts to defund the Affordable Care Act would have reduced CDC funding by a further 8 percent. Congress (primarily due to the efforts of Democrats) ultimately restored funding removed in Trump’s budgets. So these cuts did not fully occur. That said, the attempted cuts show the Trump Administration’s preference for disease preparedness erosion. In the end, Trump leadership was still corrosive to the CDC. According to a report provided by the Environmental Data and Governance Initiative:
“President Donald Trump has repeatedly undermined science-based policy as well as research that protects public health. That undermining has eroded our government’s capacity to respond to the coronavirus — from the White House itself to the labs and offices of the Centers for Disease Control (CDC), the federal government’s lead agency for science-based public health. The Trump administration’s widely-reported disbanding of the National Security Council’s directorate charged with global health has, according to many experts, hobbled the United States’ efforts against this pandemic.”
It was a hobbling that not only made the U.S. less prepared, it also set the global field — allowing any new epidemic outbreak to proceed undetected longer, to expand more rapidly into epidemics due to lack of disease response personnel, it disrupted global communications on the issue of illness, and it cost us dearly in both needed response time and lives of those who would not have been infected otherwise.
Ignoring the Severity of the Threat and Confusing the Public
The Trump Administration’s adversarial relationship with the front line soldiers in the global war on infectious disease early-on quickly morphed to a brazen denial of both the threat posed by the disease itself and the need for a strong response once it did emerge.
The timeline for these initial response failures — both a failure to take the threat of the virus seriously and communicate that seriousness to the public and the failure to provide adequate testing (next two chapters), contacts tracing, containment and isolation early on — occurred during January, February, and early to mid-March of 2020 as the disease first mostly ravaged China, then appeared overseas at first in large numbers in places like South Korea (high case numbers were, in part, due to an aggressive testing regime resulting in a clearer outbreak picture there) and then Iran with small numbers of cases elsewhere. By the end of February, it was clear that Italy was seeing uncontrolled spread of COVID-19 as well (with around 2,000 reported cases at the time). And by early-to-mid March it was apparent that both the US and large swaths of Europe were in the same boat.
Painting False Comparisons with Seasonal Flu and “Moving to Zero” in a Few Days — Trump’s Long March of Misstatement
Trump’s downplaying statements began in January and continued on through mid-March. On January 22nd, Trump stated to CNBC “We have it totally under control, It’s one person coming in from China, and we have it under control. It’s going to be just fine.” This initial major statement came notably late — weeks after first warnings (December 31) from China and WHO, and five days after CDC, in an almost unprecedented move, sent 100 disease screeners to U.S. airports. Trump’s statement was also apparently contradictory to CDC’s own statement on January 21st in which Dr. Nancy Messonnier noted “We do expect additional cases in the United States and globally.”
On January 23rd, CDC advisers reported to CNN that they were concerned that China hadn’t released enough basic epidemiological data about the virus. The next day, Trump apparently contradicts CDC again tweeting his praise for the Chinese government’s transparency and saying “China has been working very hard to contain the Coronavirus. The United States greatly appreciates their efforts and transparency. It will all work out well…” By the next day, on January 25, there are 1,000 global confirmed cases of COVID-19. By the 26th of January, China reported that the disease can infect people and be contagious before displaying symptoms.
On January 30, 7 cases have been confirmed in the United States but the country is starting to show its woeful lack of testing capability (more on this later), the World Health Organization declared a public health emergency of international concern, the U.S. State Department issued a ‘do not travel’ warning for China. Trump states on the same day: “We think we have it very well under control. We have very little problem in this country at this moment — five — and those people are all recuperating successfully.” This under-counted the official number and stood in contradiction to WHO and U.S. State Department warnings. On January 31, Trump barred many travelers from China. The Administration will later hold up this single, disorganized, inadequate by itself, and too late in retrospect action, as a ‘strong response.’ According to the New York Times, more than 430,000 Chinese still made it to the U.S. despite Trump’s travel ban (40,000 of which arriving after the ban was instated). Trump would later try to turn the blame for the virus onto the Chinese people, in statements that many described as race-baiting and which were reported to have set off a wave of acts of violence against Asian people living in the U.S.
By February 6, the virus was rapidly spreading with 25,000 known cases worldwide. In the following days, Trump would show stunning, and unfounded, optimism stating on February 7 that China will be successful in fighting the virus “especially as the weather starts to warm & the virus hopefully becomes weaker, and then gone.” Infectious disease experts on the same day noted that there wasn’t yet any evidence that warmer weather would slow the virus. On February 10 and 12, Trump would repeat this unproven information stating: “looks like, by April, you know, in theory, when it gets a little warmer, it miraculously goes away.” And “as I mentioned, by April or during the month of April, the heat, generally speaking, kills this kind of virus.”

Local counties, city and state governments, were often forced to contradict myths spread directly from Trump about COVID-19 as a matter of public health and a life-saving measure. Image source: McLean County Health Department.
By February 19, the WHO was now tracking more than 75,000 confirmed cases globally. By February 24, the White House was requesting 2.5 billion in emergency aid funding due to COVID-19. At this point, there were 51 confirmed cases in the U.S. But actual cases were probably far more extensive as U.S. testing capability remained well behind the infection curve. Trump’s statement on this day was also rosy despite a very grim global and U.S. picture starting to emerge: “The Coronavirus is very much under control in the USA. We are in contact with everyone and all relevant countries. CDC & World Health have been working hard and very smart. Stock Market starting to look very good to me!” It’s also at this point that Trump began his counter-productive increased obsession over the stock market. On February 25, CDC again showed how out of touch Trump was with reality on the ground by stating that it expected to see both community spread and thousands of deaths in the U.S.
By February 26, Trump seemed bound and determined to overwhelm the dutiful reporting of infectious disease experts with utter nonsense. He made an odd comparison between COVID-19 and the flu and then he claimed that U.S. cases would be down to zero in a couple of days. For the sake of accuracy, infectious disease experts estimated COVID-19 lethality to be 10-40 times worse than the seasonal flu (as of this writing the disease has killed more than 100,000 people globally, more than 18,000 in the U.S., is the leading cause of death today in the U.S., and has a present global case fatality rate of around 6 percent or 60 times worse than typical flu). It’s also worth noting that at a time when the official CDC case count was 58, Trump falsely claimed the number was 15. Trump’s full statement is worth reading as an example of how delusional the deniers of scientific fact can become and how damaging such delusion is to our lives: “I want you to understand something that shocked me when I saw it that — and I spoke with Dr. Fauci on this, and I was really amazed, and I think most people are amazed to hear it: The flu, in our country, kills from 25,000 people to 69,000 people a year. That was shocking to me. And, so far, if you look at what we have with the 15 people and their recovery, one is — one is pretty sick but hopefully will recover, but the others are in great shape. But think of that: 25,000 to 69,000. … And again, when you have 15 people, and the 15 within a couple of days is going to be down to close to zero, that’s a pretty good job we’ve done.”
The next day, on February 27, there were 60 confirmed U.S. cases of COVID-19. Trump at this time was still living in the cloud of his self induced denial euphoria. His statement for the day was: “It’s going to disappear. One day it’s like a miracle, it will disappear.” On February 29 the refrain for Trump continued at the Conservative Political Action Conference in Maryland when he stated: “And we’ve done a great job… Everything is really under control.” Later it was confirmed that an attendee at the same conference tested positive for COVID-19. On the same day, health officials announced the first official COVID-19 death in the U.S. Later on the 29th, Trump would claim that: “we have far fewer cases of the disease then even countries with much less travel or a much smaller population.” Of course this statement would later be proven dramatically false as U.S. cases jumped to highest in the world on a numerical basis (as of this writing, U.S. cases are now rapidly closing in on half a million).
By early March, cases were notably surging in the U.S., but testing capability still lagged, so only the most severe or high profile infections were accounted for. Regardless, on March 4, 217 cases were confirmed in the U.S. On the same day, Trump was telling people: “Yeah, I think where these people are flying, it’s safe to fly. And large portions of the world are very safe to fly. So we don’t want to say anything other than that.” At this point such statements were directly risking life — it was like telling people to go to the beach in a category 5 hurricane. Conservative followers of Trump would make similar irresponsible statements risking harm to those who listened to them in the weeks and months to follow. It’s also worth noting that the coronavirus denial messages had extended to Trump’s flu comparison by this time as well. A poll conducted by Vox from mid-March found that 90 percent of Fox viewers felt it was safe to go out even as experts were increasingly recommending stay at home policies. But looking at this litany of Trump statements, it’s little wonder how many developed such a false sense of security.
To round out this account of live-action denial, on March 6 Trump began to downplay the lack of testing availability claiming: “Anybody that wants a test can get a test. … The tests are all perfect, like the letter was perfect, the transcription was perfect, right?” This as many Americans with symptoms were forced to wait in long lines only to be turned away when asking for a test. And by March 9, Trump is again making the false equivalency comparison with the seasonal flu: “So last year 37,000 Americans died from the common flu. It averages between 27,000 and 70,000 per year. Nothing is shut down, life & the economy go on. At this moment there are 546 confirmed cases of CoronaVirus, with 22 deaths. Think about that!”
We’ll pick up the thread of Trump misstatement in a later chapter. For now, we will mercifully break from his ongoing and delusional screed to take a look at how the Administration failed so miserably to provide the much-needed test kits that could have helped to contain COVID-19 in the U.S. even as the disease rapidly spread. To look at what could have been and to try to learn from the successful responses of other nations.
(UPDATED to include more information on Trump’s China travel ban in late January.)
Up Next: Effective Containment — How South Korea’s First Coronavirus Wave was Halted
Share this:

Posted by robertscribbler on April 10, 2020
https://robertscribbler.wordpress.com/2020/04/10/denial-defunding-downplaying-first-covid-19-leadership-failures/
COVID-19 First Outbreak — Viral Glass-Like Nodules in Lungs
“The chances of a global pandemic are growing and we are all dangerously underprepared.” — World Health Organization in a September 18, 2019 statement mere months before the COVID-19 outbreak.
“There’s a glaring hole in President Trump’s budget proposal for 2019, global health researchers say. A U.S. program to help other countries beef up their ability to detect pathogens around the world will lose a significant portion of its funding.” — From a 2018 NPR news report.
*****
During recent years the world has swelled with new and re-emerging infectious illnesses. Ebola, HIV, and SARS were among the worst. And many were accelerated, worsened or enabled through various harmful interactions with the living world to include deforestation, the bush meat trade and the climate crisis. But these illnesses were not the only ones. Between 2011 and 2018, the World Health Organization had tracked 1,483 epidemics worldwide including SARS and Ebola. These illnesses had forced human migration, lost jobs, increased mortality, and major disruption to the regions impacted. In total 53 billion dollars in epidemic related damages were reported.

Comparison of lungs of a Wuhan patient who survived COVID-19 — image A-C — to those of a patient who suffered death from the illness — image D-F. Both image sets show the tell-tale ground glass like opacities of COVID-19 in lungs. Image source: Association of Radiologic Findings.
By late 2019, before the present pandemic, a sense of unease had appeared to settle upon the global health, threat analysis, and infectious disease response community. The Global Preparedness Monitoring Board (GPMB) convened a joint World Bank and WHO meeting during September. The meeting brought with it a kind of air of dread. At the time, various climate change related crises were raging around the world and the general sense was that the human system had become far more fragile in the face of an increasingly perturbed natural world. At the conference, members spoke uneasily about past major disease outbreaks like the 1918 influenza pandemic that killed 50 million people. About how we were vulnerable to that kind of potential outbreak in the present day.
“While disease has always been part of the human experience, a combination of global trends, including insecurity and extreme weather, has heightened the risk… The world is not prepared,” GPMB members warned. “For too long, we have allowed a cycle of panic and neglect when it comes to pandemics: we ramp up efforts when there is a serious threat, then quickly forget about them when the threat subsides. It is well past time to act.”
And they had reason to be uneasy, for even as global illnesses were on the rise in the larger setting of a world wracked by rising climate crisis, reactionary political forces in key nations such as the United States had rolled back disease monitoring and response capabilities. It basically amounted to a withdrawal from the field of battle against illness at a time when those particular threats were rising and multiplying. And the responding statements of increasingly loud concern coming from health experts and scientists, ignored or even muzzled by the brutally reactionary Trump Administration, would end up being devastatingly prophetic.
Live Animal Markets Again Suspect
“We do not know the exact source of the current outbreak of coronavirus disease 2019 (COVID-19). The first infections were linked to a live animal market, but the virus is now primarily spreading from person to person.” — CDC.
*****
If the story of how SARS first broke out in 2002-2003 is not fully understood, then we know even less today about how the second strain of SARS (SARS-CoV-2 or COVID-19) made its way into the human population. What we do know is that the disease is closely associated to a coronavirus found in bats, that the disease transferred from bats or animals ecologically associated with bats and the virus (such as pangolins or civets) to humans through some vector, and that live animal markets remain high on the suspect list. According to recent scientific reports, an intermediate host such as a pangolin, a civet, a ferret, or some other animal like the ones sold in wet markets probably played a role. Chinese health experts also identified a seafood and wildlife market in Wuhan as the original source of the new illness in January.
Regardless of its zoonotic genesis, COVID-19 made its leap into the human population sometime during late November or early December of 2019 in Wuhan, China where it began to spread. At first the spread was relatively slow. Or it seemed slow, due to the fact that the initial source of the infection was small — possibly just one person. But viral spread operates on an exponentiation expansion function. And like its cousin SARS-CoV, COVID-19 was quite transmissible — generating about 2.2 persons infected for each additional new illness.
Wuhan Suffers First Outbreak
At the time, no-one really knew how rapidly the illness spread. Some early reports of the disease seemed to indicate that it was easy to contain. That it wasn’t very transmissible. These accounts would prove dramatically wrong in later weeks. But this early confusion about the risk posed by COVID-19 did hint at its nasty, sneaky, back and forth nature. About how it lulled the unprepared and the overconfident into a sense of false security early on. It also would later show that slower responses to the illness in its ramp-up phase would prove devastating.
By December through mid-January, Wuhan was dealing with an uptick in pneumonia-like infections. Having experienced SARS illness before, the region was put on alert after getting days of indicators that all was not right. These response efforts have been criticized as slow. How it happened is also opaque. One reason is that China was rather close-lipped about the outbreak’s rise on its soil at first. But another reason (an arguably much greater one) for this lack of clarity is due to the fact that many U.S. disease monitors charged with providing reports about the infectious disease situation on the ground in China and various other countries were removed by the Trump Administration in the years and months leading up to the outbreak.
Despite not providing a clear early picture of the outbreak, China did start to rapidly and effectively respond during December and January. In December, researchers received samples of the disease which they identified as a new coronavirus infection — naming it SARS-CoV-2. Once samples were available, both China and the World Health Organization (WHO) swiftly and dutifully produced tests to detect the illness. As of late January of 2020, China had 5 tests for COVID-19. At the same time, WHO began deploying tests to countries and by February the global health agency had shipped easily produce-able tests to 57 countries. This early availability of testing capability provided by WHO would prove crucial to the effective infectious disease responses of many countries in the follow-on to China’s disease outbreak.
Viral Glass Like Nodules in Lungs
Back in Wuhan and in larger China, it was becoming apparent both how deadly and how transmissible the new SARS was. From mid January 23 through February 18 — over a mere 26 days — the number of reported cases rocketed from around a hundred to more than 75,000. About ten times the total cases of the first SARS outbreak in 2002-2003. This even as China shut down large regions of the country, putting the whole Wuhan region on lock-down, and setting up dedicated COVID-19 testing and treatment centers. Notably, the new SARS-CoV-2 had become not only a serious threat to China. It was now a significant threat to the globe — one unprecedented in the past 100 years. A threat on a scale that disease experts had warned of during late 2019. One that if it broke out fully was more than capable of mimicking the 1918 flu pandemic’s impact and death tally.
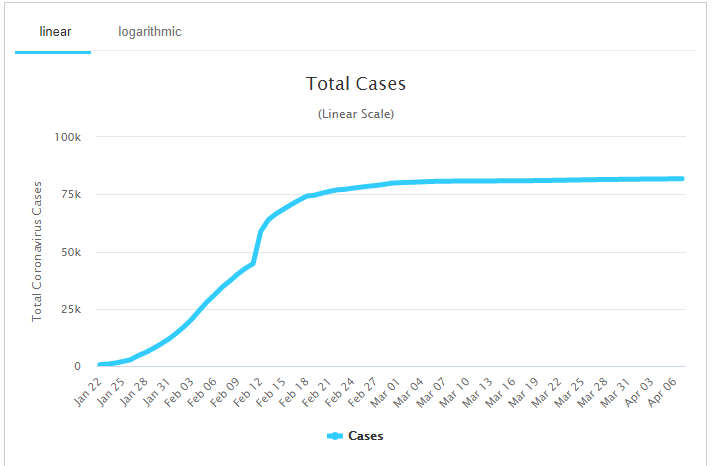
After rapid growth in COVID-19 cases in China, a strong national response has limited the first wave of outbreak in that highly populous country to just over 80,000. Image source: WorldoMeters.
The disease, which had first been seen by some as mild and easy to contain, had taken hold to great and grim effect. It produced direct and serious damage to people’s lungs. China’s dedicated mass testing centers quickly adapted to look for the tell-tale and devastating signature of COVID-19’s progress in the human body. A kind of viral glass like set of nodules that appeared plainly in scans of victims lungs.
As devastating as the disease was to individual bodies, it hit community bodies hard as well, producing mass casualties as about 15 percent of all people infected ended up in the hospital. A large number of these hospitalized cases required intensive care support (ICU) with ventilators and intubation to assist breathing. This put healthcare workers at great risk of infection themselves — because as with SARS — COVID-19 was not containable in the hospital setting without protective gear and masks (PPE). Early indications were that the lethality rate in China was around 2-3 percent or 20 to 30 times worse than the seasonal flu. Present closed reported case mortality for China now stands at 4 percent with 3,333 souls lost.
The progress of COVID-19 in an infected person was itself rather terrifying. Its ‘milder’ expression resulting in severe flu and pneumonia like symptoms with a number of other bodily responses to include serious spikes in blood pressure along with a manic variance in symptom severity. In hospital cases, victims often struggled to breathe to the point that they required oxygen. If the disease progressed, it produced serious inflammation — filling up lungs with fluid requiring support with machines for breathing. Late stage COVID-19 also attacked the body’s organs with inflammation, resulting in a need for multi-organ support in the worst cases.
Massive Outbreak of a Terrifying Illness
It was a nasty, terrible thing. It brought China to its knees — despite what ended up being a strong overall response by the country. At present, China is still recovering, still going slow with certain sectors of its economy despite limiting new cases to less than 100 per day.
The first outbreak in China was extraordinary in number of persons infected. So large as to be extremely difficult to contain through a well managed global response. But the response from key nations like the U.S. was not well managed. So through various contacts and travel vectors within the human system, this serious illness made its way out to the rest of the world. For the diligent contacts tracing and isolation, the early detection and response by international disease experts that had contained Ebola and the first SARS outbreak had been both hobbled and overwhelmed.
Up Next: Denial, Defunding, Downplaying — First COVID-19 Leadership Failures
Share this:

Posted by robertscribbler on April 8, 2020
https://robertscribbler.wordpress.com/2020/04/08/covid-19-first-outbreak-viral-glass-like-nodules-in-lungs/
The Emergence of Severe Acute Respiratory Syndrome (SARS)
“The message we are getting is if we don’t take care of nature, it will take care of us.” — Elizabeth Maruma Mrema, Acting UN Executive Secretary on the Convention on Biological Diversity.
“It boggles my mind how, when we have so many diseases that emanate out of that unusual human-animal interface, that we don’t just shut it down. I don’t know what else has to happen to get us to appreciate that.” — Dr. Anthony Fauci on live animal markets, aka wet markets, in Asia and elsewhere.
“The term wet market is often used to signify a live animal market that slaughters animals upon customer purchase.” — X. F. Xan
“This is a serious animal welfare problem, by any measure. But it is also an extremely serious public health concern.” — Kitty Block, President and CEO of the Humane Society of the United States.
*****
As we come closer to the present time, to the present COVID-19 Climate of Pandemic, we run into illnesses that are more mysterious. HIV, for example, has been the object of intense investigation and scrutiny for many decades now. So the level of knowledge about how HIV emerged is quite rich. Less so with Ebola, but that infection is still moderately well understood.
SARS — Another Novel Illness
With the newer SARS illness — short for severe acute respiratory syndrome, the well of scientific understanding from which we can draw is far more shallow. But it is certainly relevant. For the present global pandemic which now has paralyzed our entire civilization and which threatens to take so many of our lives resulted from the second strain of human SARS to emerge in our world.
What we do know is that the SARS virus is another new zoonotic illness. The first strain of SARS broke out in a 2002 epidemic in China that then rapidly spread. It emerged from a family of coronaviruses. A set of viruses that typically cause mild respiratory infections in humans. But SARS virus is not mild. It is quite often severe — resulting in hospitalization in a high proportion of cases. It also shows a much higher lethality rate than typical illness.
SARS comes from a lineage, like HIV and Ebola, that had previously thrived in the hotter regions of the globe. It was harbored in tropical and subtropical animal reservoirs. It emerged at a time when animal sicknesses were likely amplified by direct environmental stresses caused by forest clear cutting, human encroachment, and the broader sting inflicted by the climate crisis. The novel awakening of SARS was, finally, yet another case where harmful contact with sick animals resulted in a transfer of a new illness to human beings.
Coronaviruses in Hot-Bodied Bats in a Hot Weather Region
The first strain of human SARS illness was genetically traced back to a coronavirus ancestor in horseshoe bats — a tropical and subtropical bat species — in 2002 by Chinese researchers. Like the Ebola Virus and HIV before it, SARS-like illness circulated through various species in tropical and sub-tropical environments in a traditional reservoir long before transferring to human beings.

The primary range of horseshoe bats is paleo-tropical. Horseshoe bats, according to genetic research, are an animal reservoir of SARS virus. Image source: Paleo-tropical environment.
Studies note that bats are a reservoir for a great diversity of coronaviruses. The bat anatomy is a warm one in a hot weather environment — subject to constant exercise and exertion in regions where it’s not easy to cool off. Elevated body temperature is a traditional mechanism for fighting infection. So these viruses have to constantly adapt and mutate to keep hold in the bat population.
At some point, one particular strain of coronavirus jumped out of the bat population and into another animal species. A paper in the Journal of Virology suggests that the genetic split from bat cornaviruses and SARS occurred some time around 1986 or 17 years before the 2002-2003 outbreak. At that time, it is thought that this hot weather illness from hot-bodied bats had moved to another, intermediary, animal host.
SARS in the Little Tree Cats — Palm Civets
The first emergence of SARS is thought to have occurred when palm civets — a kind of Southeast Asian tree cat — consumed coronavirus inflected horseshoe bats. The civets typically dine on tree fruits. But as omnivorous creatures they also eat small mammals. In this case, civets are thought to have eaten sick bats and become sick themselves.

- The Palm Civet of Southeast Asia — hunted as bush meat for the Asian wet markets. A practice suspected for transferring SARS from bats to humans. Image source: Black Pearl, Commons.
Palm civets live throughout much Southeast Asia. Inhabiting a swath from India eastward through Thailand and Vietnam, running over to the Philippines and southward into Indonesia. A tree-dwelling creature, they prefer primary forest jungle habitats. But they are also found in secondary forests, selectively logged forests, and even parks and suburban gardens. All of which overlap the environment of horseshoe bats and their related coronavirus reservoir.
The leap from bats to civets and its development into SARS probably didn’t occur suddenly. Many civets probably consumed many sick bats over a long period of time before the coronavirus changed enough to establish itself. But at some point in the 1980s, this probably occurred.
From that point it took about 17 years for the virus to make its first leap into humans. How the virus likely made this move is eerily familiar — taking a similar route to the devastating HIV and Ebola illnesses.
Wet Markets — Butcheries For Asian Bush Meat
A major suspect for the source of this particularly harmful contact is the Chinese wet market system. A wet market is little more than a trading area that contains, among other things, live and often exotic animals for sale as food. A person entering a wet market is confronted with thousands confined live animals. They can point to a particular animal and a wet market worker will butcher the creature on the spot.
It’s literally a very bloody business. The butchering occurs in open air. Blood and body fluids can and often do splatter anywhere. As a result, the floors are typically wet from continuous drippage and, usually partial, cleaning — which is how the market derives its name.
Palm civets can often be found in wet markets as food in China. Trappers for the wet markets range the Southeast Asian jungles bringing in civets by the thousands. The civets were reservoirs for SARS virus. They were slaughtered in the messy markets. People were exposed. In 2002 and in 2019 they got sick.
Though palm civets have been identified by many avenues of research as a likely source of SARS, raccoon-dogs — whose meat was sold in wet markets — were also shown to be SARS type virus carriers. These animals have a similar diet to that of civets, share their habitat and were similarly vulnerable to infection from the bats. In addition, pangolins — a kind of scaly anteater — have been identified as a possible carrier of the SARS-CoV-2 virus. And pangolin meat is also sold for consumption in Vietnam and China.
Given our knowledge of how zoonotic illnesses move in animal populations, it’s possible that multiple species are involved in the ecology of SARS and related coronaviruses. In essence, there is a strange and ominous similarity between wet markets in Asia and the bush meat trade in Africa. They are both means of moving jungle meats from animals (who may be reservoirs for novel illnesses) in tropical regions into the human population. Often in a fashion in which the treatment and preparation of the meats to be consumed is haphazard and unregulated.
First SARS Outbreak — 2002-2003
Ultimately, the disease percolating through likely stressed natural systems found its way into the human population in late 2002. The epicenter was Guangdong Province in China where the highest proportion of early SARS cases by a significant margin (39 percent) showed up in people in the live animal food trade. In other words, people who butchered animals or worked closely with those who butchered animals.
The initial infections, which were traced back to November in China, resulted in spikes of pneumonia incidents in local hospitals. The cause — a then unknown illness that was later called SARS. SARS was another terrifying illnesses. Its symptoms could emerge rapidly or slowly over a couple of days or weeks. It could mimic flu-like symptoms before suddenly surging into a terribly lethal illness that attacked the lungs — rendering victims unable to breathe under their own power. At first, case fatality rates (the percentage of people who died as a result of SARS) ranged from 0-50 percent. The ultimate recorded fatality rate from the initial outbreak in 2002 would settle at 9.6 percent or about 100 times more lethal than seasonal flu.

Cumulative reported SARS-CoV cases during the 2002-2003 outbreak. Note that early case reporting was incomplete. Image source: Phoenix7777 and WHO.
From the point of early infections, patients then passed on the virus to healthcare workers and others. Though SARS was not as crazy lethal as HIV and Ebola on an individual basis, it was quite infectious. Meaning it was much easier to pass on to others than either of those earlier emerging zoonotic illnesses. This higher transmission rate resulted in a greater risk that more people would fall ill from SARS over a shorter period of time — exponentially multiplying the virus’s lethal potential.
Transmission to workers in hospitals and care facilities was notable as typical sanitation procedures were not enough to limit virus spread. In hospital settings, the transmission rate for this first SARS illness (the number of people each infected person then got sick) was between 2.2 and 3.7. Outside of sanitized settings, the transmission rate ranged from 2.4 to 31.3. A particularly highly infectious patient, called a super-spreader, resulted in a mass spread of illness to workers at Sun Yat-sen Memorial Hospital in Guangzhou during January of 2003 and subsequently to other parts of China’s hospital system. Masks and protective gowns (PPE) were ultimately shown as necessary to contain SARS infection in hospitals.
China’s early failures to report on the 2002 SARS outbreak resulted in a somewhat delayed international response. But by early 2003, the World Health Organization was issuing warnings, advisories and guidance. Disease prevention agencies within countries issued their own responses including diligent contact tracing and isolation protocols. The containment response both within and outside of China was thus in full swing by early 2003. This action likely prevented a much broader pandemic. That said, a total of 8,096 cases were reported — 5,327 inside China and 2,769 in other countries. With the vast majority of cases occurring in China, Hong Kong, Taiwan, Canada, Singapore and Vietnam. In total, out of the 8,096 people reported infected during this first SARS outbreak, 774 or 9.6 percent, perished.
SARS-CoV-2 Tsunami on the Way
Unfortunately, infectious diseases show no mercy to fatigued and degraded infectious disease responses. They lurk. They mutate. In their own way, they probe our defenses. They are capable of breaking out to greater ranges when diligence, ability, or will to protect human life wanes among leaders. And a smattering of SARS cases reported during the 2000s following the 2002-2003 outbreak continued as a reminder of its potential. So as with HIV and Ebola, we face waves of illness with SARS. With the next outbreak resulting in a global pandemic that will likely infect millions and kill tens to hundreds of thousands during 2019-2020.
Up Next: COVID-19 First Outbreak — Viral Glass-Like Nodules in Lungs
Share this:

Posted by robertscribbler on April 7, 2020
https://robertscribbler.wordpress.com/2020/04/07/the-emergence-of-severe-acute-respiratory-syndrome-sars/
Harmful Contacts with our Living Earth and Redounding Shots Across the Bow
About two-thirds of all infectious diseases in humans have their origins in animals. Scientists say the ability of a virus to mutate and adapt from animals to the human system is very rare, but the expansion of the human footprint is making that rare event much more likely. — Jeff Berardelli
Contact — the state or condition of physical touching.
Harmful or unwanted contact — an assault.
Redound (archaic) — to come back upon; rebound on.
*****
How do you get sick from a virus? In the most simple sense, the virus touches your skin, your eye, the inside of your mouth, your blood or some other part of your body. It makes contact. Then it gets inside to do its damage. Often, this is through some action that you take. Some voluntary, some involuntary. Breathing, moving, picking up objects, putting contaminated clothes or blankets on or venturing into environments where other carriers of the virus can touch you. Or even, in a broader sense, disturbing the virus carriers and changing their environment is such a way that makes it easier for them to literally come to your home community to roost.
Contact.
In the last chapter we briefly explored how the world houses many, many potential, new, and re-emerging illnesses. Kept away from humans in mostly safe or remote places. We also briefly looked at how those illnesses are expanding. In this chapter, we will take a deeper dive into the second part. To look at how some harmful elements and activities within of our civilization have wrecked some of those safe places, how they’ve gotten us into what amounts to a brutal embrace with the places and beings in living nature that are reservoirs to those illnesses. How in this epic and global struggle, often bad actions and behaviors have shaken some illnesses loose. How it’s all gotten many of us sick.
That’s our present and recent history. One of harmful contact. Of touching and grasping for things best left undisturbed. And how it’s getting worse. How the general disturbance is rippling outward and bounding back.
We’re living in a time of an explosion of new illness or the re-emergence of old illnesses previously thought contained onto the global scene. How this has happened first became a major part of the discussion among health and epidemic experts since around the 1980s. For at the time, we experienced one of our initial major warnings that diseases may be dedounding onto expanding global civilization. And this first warning came from a terrifying new illness. For HIV humbled a global health corps that until that point had seen a long string of victories arising from the advances in medical science during the 19th and 20th Centuries.
HIV — Major Warning Shot to the Global Health System
HIV heralded an ominous new era. One where victory against infectious illness was less certain or at least came much slower and at a much higher price than earlier medical science victories might have given us hope for. One in which disrupted, damaged, or harmfully contacted life (and its supports) appears to return a toll on humankind as various enormous and harmful activities spread — burning, deforesting, killing and eating, and polluting their way across the globe.

3D rendering of HIV. Image source: National Foundation for Infectious Diseases.
Since its first outbreak as a pandemic during the early 1980s, HIV has infected over 75 million people of which around 32 million have died as a result of an illness that jumped to human beings from primates. Many deaths occurred early in the pandemic outbreak as first treatments were mostly ineffective. But even today HIV kills between 500,000 and 1,100,000 people each year (770,000 during 2018).
HIV originated in the broader African rainforests. There its progenitor reservoir existed as semian immuno deficiency virus (SIV) in the great apes and monkeys of the jungle for more than 10,000 years. All without transferring to humans until very recently. Our best present understanding is that the ultimate zoonosis occurred due to the bush meat trade in Africa which produced multiple contacts between SIV in apes and the blood of humans.
Hunting, Rubber and Bush Meat
The story of the bush meat trade is one that should be eerily familiar to those researching the climate crisis. Because it is also a story of forced displacement of human populations which then results in a harmful interaction with the natural world and subsequent damaging upshots. In the period from around the 1880s to the 1920s, sub-saharan Africans were forced from their native rural homes in droves as waves of Europeans descended on the jungles of Africa.
The Europeans wanted elephant tusks from the hunting trade to be sent home to Europe. They wanted rubber vine sap for industrial uses. They wanted to commoditize the jungle for these and other products. But often the Europeans didn’t have the manpower or local knowledge to conduct effective hunting expeditions into the jungle without the help of native populations. And they needed a local labor force for the rubber vine trade. Tribal Africans were pressed into service for the expeditions and the industrial exploitation of jungle plant products, often at the point of a gun.
This was a kind of mass invasion of the jungle in which abused and often under-nourished natives needed a new food source to survive. Rural subsistence agriculture wasn’t a possibility for a constantly mobile porter in an elephant hunting expedition. Nor was it for rubber plant harvesters or those newly impressed into factory work in burgeoning cities.

“At this bushmeat market in Pointe Noire, a butchered chimpanzee is shown in the middle of the photograph, along with other smoked and fresh meat. It has been theorized that SIV moved from chimpanzees and sooty mangabeys to humans—evolving into pathogenic HIV-1 and HIV-2 respectively–through exposure to primate blood, most likely as a result of the bushmeat trade. The HIV-1 group M epidemic likely began in the region of Kinshasa, Democratic Republic of Congo. Although wild chimpanzees are not found in the immediate vicinity of Kinshasa, the city is situated on the Congo River, which allowed for the easy transport of SIV-infected bushmeat and of infected humans from rural to urban areas.” Image and caption source: Physicians Research Network and the Goldray Consulting Group.
So a kind of shadow trade in bush meat arose. Porters on hunting expeditions would opportunistically kill and butcher the jungle animals they came into contact with to supplement their diets. It was an ironic and ominous outgrowth of the abuse handed down to the native Africans by the Europeans. It was almost as if they’d been corrupted by the hunting and killing they were forced to take part in such that it became a new means of survival for them.
The Monster that Lives in the Jungle and the Monster that Lives in Us
Various strains of SIV lived in the blood of apes and monkeys in Cameroon and Sierra Leone. Porters and laborers driven into the jungle killed and ate their hominid relatives to survive the European expansion into Africa and its subsequent exploitation. Hunted chimps and monkeys fought back. They bit. They flung feces. Tired porters and laborers hunting chimps after endless hours of work made mistakes. They missed when cutting chimp meat off of bones. They under-cooked bloody meat. They cut themselves with bloody knives containing the blood of their hominid fellows. The SIV living in the blood of the monkeys and apes its way into the blood of the porters and laborers. It happened many, many times.
At first, SIV was a mild virus in humans. It didn’t live well in the new host. But viruses are weird. Like life, they mutate. They change. They adapt to new environments. If there is one prime directive a virus has in its intrinsic design it is to self-replicate. At some point in all the butchering and eating and messy cutting or in the conflicts between the people hunting the apes and monkeys for food and the fighting creatures struggling for very existence, there was an SIV transmission into humans that caught fire. Changing from the mild SIV to the raging and lethal human immuno-deficiency virus that we know today.
It had to have happened multiple times. We know this, in part, because there are not one but two progenitor strains of HIV — HIV 1 which links back to apes and chimps in the Cameroon region and HIV 2 which links back to Sooty Mangabays in the Sierra Leone and Ivory Coast region. A grim bit of evidence pointing to how widespread the harmful contact was that resulted in the virus’s leap into humans. The point in time at which the consistent leap was made is thought to have occurred in the pre-World War 2 period — possibly as early as 1908.
Once the leap happened, the machine of exploitation in Africa that the colonialists had set up then served to help spin the virus out into the broader human population. Industrial centers and related communities had sprung up around the animal products and jungle harvesting trades. And in those centers prostitution of various kinds was rampant. Already established human illness such as syphilis, chlamydia and gonorrhea became widespread in Africa. These illnesses assisted the spread of HIV into hundreds of people by the mid 20th Century. This created a consistent viral HIV reservoir in humans from which the major pandemic later emerged.
Ebola — Novel Jungle Hemorrhagic Fever
If HIV was the first known serious illness to arise through harmful human interactions with ancient tropical and subtropical disease reservoirs, it became sadly apparent early on that it would not be the last. More human beings were coming into contact with the old animal disease reservoirs moving from previously sequestered habitats than before.

An electron microscope image of Ebola virus. Image source: CDC.
Cities were extending into the jungles, animals carrying illnesses foreign to humans were moving into those cities. Deforestation and slash and burn agriculture was displacing them, driving them. And in most new places that the animals moved there were human beings as well. A new harmful interaction, the climate crisis driven by fossil fuel burning, was also beginning to heat up the world. This served as a new pathway for expansion — increasing the habitable range for creatures used to hot weather and typically averse to cooler climes. This greatly increased and continues to increase the spatial range of tropical and semi-tropical illnesses capable of infecting people.
Of the jungle fevers that arise from the hot regions of the world, that are carried by animals that live in this heat, the viral hemorrhaigc fevers are perhaps some of the most terrifying. Like HIV, they are seriously lethal — tricking the body’s immune response in a way that enables them to multiply out of control. Directly attacking the body’s linings, they thus cause such great cell death that they effectively blow holes in tissue. This breaks down the body’s integrity causing loss of fluid and ultimately bloody hemorrhage.
From Viral Brush-fire to Conflagration
The first instances of Ebola occurred in 1976— in Sudan and then in Zaire. These initial infection outbreaks were highly lethal and terrifying to the local populations effected. Of the 284 people suffering from the Sudan strain of the virus, 151 died. In Zaire, 280 out of the 318 infected souls (88 percent) perished. For a relatively short-lasting infection, Ebola was amazingly lethal. Though later, less deadly strains emerged, many of the outbreaks to follow would continue to kill a surprising number of those afflicted. Presently, the World Health Organization estimates the lethality rate for Ebola, overall, at 50 percent. Sudan and Zaire both hosted different strains (SUDV and EBOV) of the same virus — Ebola — which was named after the river region from which it emerged.
It is still not fully known how the deadly Ebola virus first made its leap into humans from animals. But it is well known that tropical fruit bats, porcupines, and primates — yes our poor hominid relatives again — can carry the virus. As with HIV, the harmful bush meat trade is one of the key suspects. Although with Ebola, there are many other possible modes of zoonosis from animals to humans.
The virus is more transmissible than HIV, though less so than many other illnesses, such that direct contact with blood, secretions, organs or other bodily fluids of infected people or animals, and with surfaces and materials (like bedding and clothing) contaminated with these fluids can result in sickness. It is thought that eating fruits partially eaten by fruit bats, food contaminated by bat or other infected animal feces, or consuming bush meat are all means of animal to human transfer of the illness.

Initially, the bush meat trade was a prime suspect for transmission of Ebola to human beings. Presently, it’s understood that other contacts with infected animals or their bodily fluids may transmit the virus. Also, at first, Ebola primarily impacted areas bordering the jungle. But in recent outbreaks, major population centers have been impacted. Image source: Ebola Virus Ecology — CDC.
Notably corpses of both humans and animals who were killed by the illness remain infectious for some time — requiring special burial. The disease typically spreads from human to human through direct contact with the blood, semen, saliva, vomit or other body fluid of infected persons. Surfaces contaminated by these fluids are also a means of infection. The virus is thankfully fragile in air, but splashing with droplets can transfer illness. And the virus is known to live in droplets on surfaces for up to 3 days.
After Ebola first burst onto the scene in 1976, there was a long hiatus of epidemic outbreaks in humans. Some thought, hopefully, that the disease had faded back into its tropical environs. But in 1995, nearly two decades after its first emergence, the virus broke out among humans in Zaire again — this time infecting 315 and killing 254. Subsequent outbreaks occurred every five years or so leaping to Uganda in 2000 (425 cases, 224 deaths), the DRC in 2003 (143 cases, 128 deaths), again in DRC in 2007 of a less lethal strain (149 cases, 37 deaths) and in 2012 in both Uganda and DRC yet again in three separate outbreaks (Uganda — 31 cases, 21 deaths; DRC — 57 cases, 29 deaths).
Thus far, outbreaks of the novel illness had been relatively small if intense viral brushfires. And, though lethal, the virus was thought be inhibited in transmission. A major outbreak spanning from 2013 through 2016 would belie that impression. Looking back, the illness had mostly been confined to small settlements bordering jungle regions in the 1976 to 2012 timeframe. But in 2013 and 2014 the virus, possibly through the enlarging span of its animal reservoirs, penetrated into more densely populated urban and city environments. From these more packed regions the virus would explode to rage out of control for years — consuming many thousands of human lives.
The West African outbreak which would hitherto dwarf all previous episodes of Ebola began in late 2013. Then, a one year old child perished from Ebola infection from an unknown source. Afterward, the disease rapidly spread through her community in Guinea, out into the local region and then on through the nearby countries of Liberia and Sierra Leone. What precipitated was a global health emergency that reached catastrophic proportions by summer of 2014 with the virus overwhelming the medical capacity of impacted countries. At this point the illness threatened to go global — with a handful of cases leaping to neighboring countries in Africa and even transferring overseas. But intense contact tracing and strict isolation both inside and outside the virus hot zone was largely responsible for preventing further spread.
By the end of the outbreak in 2016, an estimated 28,646 infections had occurred of which 11,323 were reported to have died. Ebola had risen from the ranks of a fringe if rather scary illness cropping up on the outer edges of society to an illness striking directly at the bones of global civilization. It had shown its ominous potential.
Subsequent outbreaks in 2017 and 2018 in DRC and Equateur Province mirrored previous less widespread infections. But a new outbreak that began in 2018 in the Kivu region of DRC and extends to today is considered a global health emergency by WHO. This particular outbreak as of 29 March, 2020 is reported to have infected 3453 people of which 2273 have died.
Warning Shots Across the Bow
Both Ebola and HIV served as early warning shots across the bow of global civilization. Visible signals that the risk of catastrophic emergence of new infectious illness was on the rise. That our harmful contacts with the natural world were the primary source of this rising risk. And that many, many more human souls may be at stake. These two novel illnesses were not the only major emergences to occur in this time. In fact, a plethora of new and re-emergent sicknesses have come onto the global scene over the past four decades. But they both represented the ominous character of the larger risk human beings now faced. They also foreshadowed the follow-on emergence of SARS into a major global pandemic — which we’ll be talking about in the next chapter.N
(Up Next — The Emergence of Severe Acute Respiratory Syndrome)
Share this:

Posted by robertscribbler on April 5, 2020
https://robertscribbler.wordpress.com/2020/04/05/harmful-contacts-with-our-living-earth-and-redounding-shots-across-the-bow/
From Ancient Reservoirs
“The insidious emergence of HIV/AIDS and the lack of due attention by policymakers illustrate how some outbreaks that start subtly can grow to global proportions if they are not aggressively addressed early on.” — Dr Anthony Fauci
The Infectious Diseases Society of America recognizes climate change as a global health emergency and calls for policies responding to the intrinsic links between warming temperatures and rising sea levels and epidemic and pandemic events as well as other infectious disease threats to public and individual health. — IDSA
The climate system of our world envelopes it.
It represents the state of our atmosphere, our oceans, and the frozen regions we rely on. It interacts with and influences all things living here on Earth.
The present changes we now experience due to a climate in crisis are far-reaching. Disruptive to the balance of life itself. Harmful or even demolishing to ecosystems. Driving species of all kinds into new environments after their old safe places have been changed, disrupted, or taken away.
This is a story that we have become sadly familiar with as the burning of fossil fuels keeps dumping heat-trapping carbon into our atmosphere — resulting in rising seas, melting ice, stronger storms, worsening droughts, expanding heat, and far larger and more dangerous wildfires.

Global examples of emerging and re-emerging infectious diseases. Even before COVID-19, they were growing more numerous. Back in the early 1990s, this map showed just one illness — HIV. To humans, quite a few are now rather new. Others are re-emerging. Many are influenced by the climate crisis in various ways. Image source: Three Decades of Responding to Disease Outbreaks — NIH.
But there is one aspect of our changing climate that is often nuanced and overlooked — how the climate crisis can influence the spread of disease itself. How a disrupted global climate can drive sickness up out of the ancient reservoirs that have harbored it throughout the ages. How it can help accelerate the spread of new illness, make us more susceptible to sickness, or cause the re-emergence of previously well-contained diseases. Given the present context of a global pandemic caused by an entirely new illness — COVID-19 — it’s crucial to take a look at generally how harmful interactions with the natural world, particularly through climate crisis, are increasing risks of new and re-emerging diseases.
Reservoirs as Illness Havens
For what we know of as illness is also a kind of life.
Bacteria are micro-organisms. Viruses are pseudo-life and life-altering. And parasites are living things that dwell within or upon other living things. Climate change can generate or worsen such illnesses by directly affecting their environments as well. Creating the conditions that facilitate the transfer of diseases from typical ranges — called reservoirs — to new hosts. Developing pathways for expanded or new (novel) infections.
An illness reservoir is any person, animal, plant, soil or substance in which an infectious agent normally lives and multiplies. A harbor for the bacteria, viruses, or parasites that cause disease.
Human beings are reservoirs for certain diseases. These could be living humans or the dead — long buried and held dormant in ancient frozen tundra for hundreds or even tens of thousands of years. It is possible that the devastating illness smallpox (Variola virus), which was recently considered eradicated, may still be harbored by frozen dead humans entombed in the permafrost. That permafrost is now thawing as the Arctic heats up.
Animals can also be reservoirs — rabies, for example, lives in bats, raccoons, skunks, and foxes. Cholera is a bacteria that lives in water. It can also live in humans and zooplankton. And there is a link between the spread of Cholera and the loss of water security — which the climate crisis risks. Anthrax lives in herd animals like sheep and reindeer. Because it is capable of developing spores, Anthrax can survive for decades in the bodies of dead reindeer and the climate crisis produced thaw of permafrost has already resulted in new outbreaks of this illness in herd animals and, in rarer possible cases, human beings. Dengue fever is a nasty virus harbored by both humans and mosquitoes. And it is worth noting for diseases which cause illness and loss of life in human beings that mosquitoes — whose range can be greatly altered by changes in climate — weigh quite heavily.
Zoonosis — The Transfer of Illness From Animals to Humans
During recent years, human beings have unfortunately seen the emergence of numerous new or novel illnesses. Many of these illnesses have arisen as the result of mistreatment of nature. Our disruption of the natural world and harmful or abusive relationships with animals appears to have done double duty in getting us ill. For a good share of the nastier new ailments have arisen as the result of zoonosis — or the transfer of diseases that previously affected only animals to human beings — involving such harmful acts.
The harmful bushmeat trade in Africa is thought to be the origin of the novel HIV virus transferring from its original reservoir in primates as SIV before mutating into a stronger illness in humans during the 20th Century to become common from the 1980s onward. Though there is little clear and present evidence that the jump from animals to humans for HIV was directly influenced by the climate crisis, the link between harmful industry and disease transfer is a bit close for comfort here. It is also worth noting that those living with HIV are among the most vulnerable to increasing extreme weather events and related disruption of human habitat and support systems driven by the climate crisis.
SARS illnesses (of which COVID-19 is a subset) and Ebola are also novel viruses in humans. As with HIV, they are likely zoonotic illnesses. This means they originated in animal host reservoirs but, through some process of contact, transferred to human beings. These viruses are still rather mysterious in that they presently have unconfirmed reservoirs. But both are reasonably suspected to be harbored by animals — with tropical and subtropical bats relatively high on the list.
With Ebola in particular (we’ll talk about some similarities between Ebola and SARS due to suspect reservoirs in the next chapter), there is a bit of an ominous interaction with the climate crisis. New modeling produced in Nature Communications suggests that under the present pathway of global heating, Ebola epidemics in Africa could occur once every 10 years — or almost twice as often as they do at present. This is because the bats and other animals that are thought to harbor the virus are expected to be driven by warming temperatures into new areas — expanding the epidemic-prone region by 20 percent.
Expanding Heat
The heating function of the climate crisis is very well understood. And, early-on, scientific research from world health and climate agencies identified the risk that more global heat posed to expanding illness. In particular, mosquitoes which are both reservoirs and vectors (agents of disease transfer) for numerous harmful illnesses are seeing their ranges greatly expand as the world heats up.
Mosquito-borne infection is an ancient and well-known threat to humankind. But it has thankfully been relegated to warmer climates. Despite knowing little about mosquito-borne Malaria, the Roman aristocrats of antiquity did know they could avoid infection by retreating to villas in the cooler hills. Away from where mosquitoes were plentiful. Unfortunately, the climate crisis is driving heat, and the mosquitoes that come with it, both uphill and into higher latitudes.
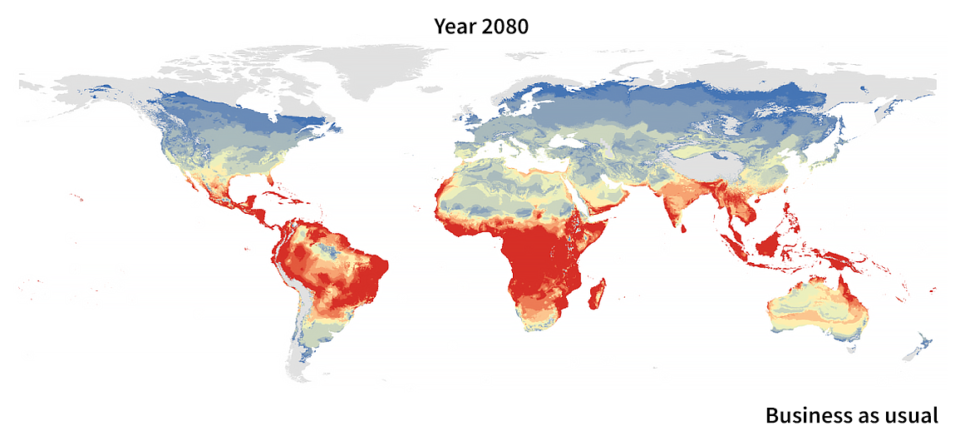
Global expansion and redistribution of Aedes-borne virus transmission risk with climate change. Ryan SJ, Carlson CJ, Mordecai EA, Johnson LR (2019).
A single populous species of mosquito — Aedes aegypti — can spread four serious illnesses. They include Dengue Fever, Zika virus, Chikunyunga and Yellow Fever. As global heating continues to be driven by fossil fuel burning, the range of this mosquito is expected to greatly expand. How much depends on how rapidly we halt fossil fuel burning and transition to clean energy (or not). But a business as usual (worst case) fossil fuel burning scenario in which the clean energy transition continues to be hobbled will bring this so-called jungle fever carrier to the Arctic by the 2080s (see image above).
There are over 3,500 species of mosquito. Most are relegated to warmer climates. In addition to the illnesses mentioned above, these insects also carry Malaria and West Nile virus among many others. And as the climate heats up, their range and their ability to transfer diseases among humans will expand.
But mosquitoes are not the only disease reservoir and disease vector species now on the move as a result of the disruption caused by climate crisis. There are many. Some which we probably don’t yet know about.
Receding Cold
If tropical heat spreading northward bringing with it flights of mosquitoes and displacing other disease carriers presents one illness expansion problem, the ongoing thaw of cold regions presents another. In particular, there is evidence that the Arctic has locked away numerous ancient illnesses that could be released in the thaw produced by climate crisis.
The Variola virus which causes Smallpox may well be sequestered in the various graves and burial mounds scattered throughout the Asian and European north. A study conducted in the 1990s detected fragments of smallpox DNA in the remains of Stone Age humans as well as people who were known to have died from smallpox during the 19th Century. Though smallpox was considered eradicated from human beings, long deceased humans frozen in the Arctic may serve as a reservoir that results in potential new infections. If such a reservoir exists, the Arctic thaw produced by the climate crisis will disturb it.
Other pathogens that may still be harbored by dead humans frozen the Arctic includes the 1918 Spanish flu (H1N1) which was found in frozen regions of Alaska. In 2007, scientists discovered Spanish flu RNA in the body of an Inuit woman who’d been buried for 75 years in the permafrost.
Anthrax is a bacteria-caused infectious disease that typically afflicts herd animals such as sheep and reindeer. But Anthrax can pass to humans that are exposed to the bacteria. In 2016, 2,000 reindeer became infected with Anthrax in the Yamal Peninsula region of Siberia. Nearby, it is thought that a reindeer killed by anthrax decades before thawed out, spreading the bacteria into the lands where the reindeer grazed. These reindeer then spread the illness to a number of human beings, including a 12 year old boy who died.
The potential for the release of both known and other as-yet unknown infectious agents from the thawing regions of our world have generated concern among top researchers. Jean-Michel Claverie a professor of microbiology at Aix-Marseilles University recently noted to BBC:
“Following our work and that of others, there is now a non-zero probability that pathogenic microbes could be revived, and infect us. How likely that is is not known, but it’s a possibility. It could be bacteria that are curable with antibiotics, or resistant bacteria, or a virus. If the pathogen hasn’t been in contact with humans for a long time, then our immune system would not be prepared. So yes, that could be dangerous.”
A Context of General Disturbance
Overall, it is likely that there are more numerous climate influences to disease transfer than mere heating and thawing. The general disturbance to the natural world generated by more extreme fires and floods, by instances of flash drought, and even by the mechanism of rising seas is likely to displace more disease reservoirs, creating previously unknown illness transmission potentials.
As far as our general scientific knowledge of illness related to or influenced by the climate crisis at this time, what we see now is likely the tip of the proverbial iceberg. And, as with all things climate crisis related, we require more research, more knowledge-sharing, more general public support of scientific discovery to pull back the veil on this particular new threat. So in conclusion of this chapter on the climate crisis relationship to human illness, we’ll depart with a statement from the World Health Organization:
Changes in infectious disease transmission patterns are a likely major consequence of climate change. We need to learn more about the underlying complex causal relationships, and apply this information to the prediction of future impacts, using more complete, better validated, integrated, models.
Up Next — Harmful Contacts with our Living Earth and Redounding Shots Across the Bow
Share this:

Posted by robertscribbler on April 1, 2020
https://robertscribbler.wordpress.com/2020/04/01/from-ancient-reservoirs/
Climate of Pandemic — Announcement and Contents

Image of COVID-19, or coronavirus 2 (SARS-CoV-2) which is a sudden acute respiratory syndrome type virus, created at the Centers for Disease Control and Prevention (CDC). Image source: CDC.
Scribbling through a Global Pandemic
The present tragedy of the COVID-19 Pandemic has impacted us all. For my own part, I am now at home under quarantine with my wife. This is a decision I have made to protect myself, my family, and my fellows here in Maryland, America, and across the world.
As many of you know, I had taken a long hiatus from climate writing to help promote clean energy as a response to the climate crisis. I did this by using the Uber rideshare platform, driving a Tesla, and sharing conversations with riders of all stripes — from business and government leaders to everyday people — as a way of raising grass roots awareness about the climate crisis and directly showing that solutions are available now to everyone.
I feel that these conversations were very effective. That I helped both raise awareness in the local community as well as among leaders and decision makers. I’ve found that it is so much easier to convey concern and caring through the medium of direct interpersonal contact vs mere words written on an electronic page or even the more adept but still far removed from the heart-to-heart media provided here on the interwebs.
But life has a way of catching up with us. Particularly at a time when our world is being shaken to its very roots by forces unwisely unleashed. We are all now isolated out of necessity. Out of safety. Out of responsibility for our fellow human beings.
Duty in Exile
So this is my task in exile — Climate of Pandemic. A combined special report and web book. A project that will explore the breadth and depth of the global coronavirus emergency. Take an in-depth look at how climate change may have helped to shake it out of an ancient viral reservoir. Reveal how the brash and brutish politics of climate change denial encapsulated the failed leadership that enabled the virus to spread like wildfire. And look at how experts are concerned that more pandemic threats may be on the way due to the great shaking up of the natural system that the climate crisis is now inflicting on our world (hopefully, I’ll be able to pick up on some other climate writing as well, but this will be my special focus for the time being).
Of course, in piercing this subject, we will likely drift into direct reporting on the emergency itself — dipping into the realms of epidemic science and disaster response. That’s OK! Because we should understand that the basic value of climate crisis response lies in both our understanding of inter-related contexts out of a sense of holistic responsibility to our world and its inhabitants.
What follows is the table of contents with links to each chapter in the new special report. At present, I have seventeen planned. But given how we are living in such uncertain and tragic times that might well expand. New links will be provided as each chapter is written. And upcoming installments will have the parenthetical (in progress) label. To quick-link this table of contents, you can click the Climate of Pandemic illustration on this blog’s side-bar and get right to catching up or reading an update.
Best to you all! Please stay safe! Please care for your loved ones! And please remember that caring for our world is also providing that much needed care and response as well.
Climate of Pandemic Contents:
- Introduction — Climate of Pandemic
- From Ancient Reservoirs
- Harmful Contacts with our Living Earth and Redounding Shots Across the Bow
- The Emergence of Severe Acute Respiratory Syndrome (SARS)
- COVID-19 First Outbreak — Viral Glass-Like Nodules in Lungs
- Denial, Defunding, Downplaying — First COVID-19 Leadership Failures
- Effective Containment — How South Korea’s First Coronavirus Wave was Halted
- The Trouble with Testing — “No Responsibility at All”
- It’s Everywhere Now — COVID-19 A Global Viral Wildfire
- No COVID-19 Did Not Stop the Climate Crisis — But it’s Interacting with it in a Bad Way
- Social Distancing and Waiting Until It’s Safe Enough to Re-Open
- A Possible Vaccine, But When?
Share this:

Posted by robertscribbler on March 27, 2020
https://robertscribbler.wordpress.com/2020/03/27/climate-of-pandemic-announcement-and-contents/
Melting Ice Everywhere — Arctic Sea Ice Extent Hit New Record Lows in Late July and Early August
If there is one word I’d use for the summer of 2019 it would be awakening. Awakening to a general public awareness of a climate crisis driven by fossil fuel burning we are now entering the throes of.

(According to NOAA, July of 2019 was the hottest July on record for the state of Alaska. This likely presages a July that will be globally the hottest July ever recorded in 2019. Much of this excess July heat was centered on the polar zones during the month — resulting in serious ice loss for both Greenland and the floating Arctic sea ice. Image source: NOAA.)
The global record hot month of June along with its related severe heatwaves, storms, and droughts have certainly served to raise the general awareness of trouble. Our new youth advocates such as Greta Thunberg and an expanding Extinction Rebellion, have certainly served to amplify the much-needed message. But vividly melting ice in tremendous volume — particularly in Antarctica, Greenland and on the ocean surface has also played its role.
The Arctic zone has seen an outrageous hotter than normal period that has extended throughout July and well into August. States and regions within or near the Arctic Circle have experienced temperatures from the upper 70s all the way into the lower 90s. Great wildfires have blanketed large sections of thawing permafrost and boreal forest — casting out smoke plumes covering as much as 4 million square kilometers at a time. Greenland saw a single day in which ice melt exceeded 11 billion tons. By volume, that’s 11 cubic kilometers — roughly equal to 11 moderate sized mountains — gone in a single 24 hour period (what does one cubic kilometer look like? See here.).
Out in the ocean waters of the Arctic, another key feature of our climate system that keeps the Earth environment stable, was getting hammered by the rising heat. For every day from July 22nd through August 9th, Arctic sea ice extent had been running in record low ranges below previous low marks set for this time of year during 2011 and 2012.
2012 in particular was a very severe Arctic melt year. Both sea ice and Greenland saw significant losses at that time. But it appears as we end the decade of the 2010s and start to enter the 2020s, Arctic summers like the one that occured in 2012 will become commonplace even as new hot outliers are more possible. For 2019 has begun to replace some of the previous worst losses seen during 2012.

(Arctic sea ice extent entered new record low ranges below the 2011 and 2012 lines during late July and into early August. By August 11, Arctic sea ice had dropped to 5.249 million square kilometers the second lowest measure for the date. Image source: NSIDC.)
As we get into August, it appears that at least some of 2012’s late season sea ice records will hold. The new August 11 measure of 5.249 million square kilometers is just above 2012’s low mark of 5.190 million square kilometers. And August 10 saw 2019 edging just above the 2012 line in the NSIDC measure.
Looking forward, the second week of August is expected to bring 1.38 C above average temperatures for the Arctic region. This is a rather significant departure for August as Arctic temperature anomalies tend to moderate during summer. And very warm ocean surface temperatures ranging well above 4 C warmer than average for large regions is likely to continue to enhance sea ice melt (see right image below).


(Greatly reduced Arctic sea ice extent [left] faces off against much warmer than normal Arctic ocean waters during August of 2019 [right]. Image sources: Uni Bremen and DMI.)
But a present lack of forecast strong weather systems that typically impact ice at this time of year such as burly high pressure ridges over the Central Arctic or major storms invading from the south may help to maintain at least some of the ice. Nonetheless, with so much heat left in the Arctic system and with sea ice perilously thin for this time of year, I’d be remiss if I didn’t say that anything can happen between now and traditional melt season end in mid September.
(Related video blog above.)
(Want to help fight the climate crisis by transitioning to a clean energy vehicle? Get 1,000 free supercharger miles at this link.)
Share this:

Posted by robertscribbler on August 12, 2019
https://robertscribbler.wordpress.com/2019/08/12/melting-ice-everywhere-arctic-sea-ice-extent-hit-new-record-lows-in-late-july-and-early-august/
What 2019’s Hottest June Ever Recorded Says About the Climate Crisis
Hint — It’s accelerating.
*****
To be a climate scientist, to read the science, or to otherwise track today’s unfolding global disaster brought on by fossil fuel burning, is to witness a historical event beyond the scope anything encountered by human civilization.

(July 14th’s record low Arctic sea ice ringed by far northern wildfires and related smoke plumes is just one signal of a rapidly heating global climate. Image source: NASA Worldview.)
Over the past Century, heat trapping pollution has forced the world to warm by about 1.1 degrees Celsius. That’s 1/4 the difference between what humans are used to and an ice age — but on the side of hot. Seas, swollen by this heat and by thawing glaciers, have risen by an average of about 17 centimeters since 1900. Nine trillion tons of ice — the equivalent to 9,000 mountains — have melted from those glaciers into our oceans. Wildfires in the U.S. now burn twice the number of acres as they did 30 years ago. Flood events are more than twice as frequent as during the 1980s. Strong hurricanes have doubled in frequency in the North Atlantic over a similar period. The Arctic’s sea ice is in full retreat.
And if we continue burning fossil fuels, this is just the beginning.
June of 2019 was the hottest June ever recorded in the 139 year global climate record provided by NASA. It was about 1.15 C hotter than 1880s averages and exceeded the past hottest June — 2016 — by a full 0.11 C margin. In climate terms, this was a big jump upward.

(Distribution of hotter and colder than average temperatures shows most of the globe sweltering under greenhouse gas induced heating. In particular, the Arctic has been hit quite hard in the most recent round of extreme temperatures. Image source: NASA GISS.)
Perhaps more importantly to the larger trend, the first half of 2019 was the second hottest first six month period on record. Meanwhile, 2019’s heat comes in the context of the past five years. All were one of the five hottest years ever recorded. And NASA GISS head Dr. Gavin Schmidt’s projection is pointing toward a potential second hottest 2019 as well. Dr. Schmidt stated as much to the Guardian, saying:
“It is clear that 2019 is shaping up to be a top-five year – but depending on what happens it could be second, third or fourth warmest. The warmest year was 2016, which started with a big El Niño, which we didn’t have this year, so a record year is not particularly likely.”
With the global climate system so large and subject to swings (produced mainly by El Nino and La Nina), consecutive hot years are a signal of accelerating global heating. A trend born out by NASA’s global temperature record. In the 1990s, decadal temperatures averaged around 0.61 C above 1880s readings. The 2000s — 0.8 C hotter. The 2010s thus far — 1.08C hotter. In other words, the global heat gain from the 1990s to the 2000s was approximately 0.19 C while the heat gain so far from the 2000s to the 2010s is about 0.28 C. A near doubling of past 0.15 C decadal temperature increases.
(Record hot July may follow record hot June…)
This apparently accelerating global heating is driven by rising atmospheric greenhouse gas concentrations. Dr Michael E. Mann noted to Mashable today:
“As we have shown in recent work, the record warm streaks we’ve seen in recent years simply cannot be explained without accounting for the profound impact we are having on the planet through the burning of fossil fuels and the resulting increase in atmospheric greenhouse gas concentrations.”
Carbon dioxide, which is the primary driver of heat gain, is now at around 411 parts per million — 37 percent higher than during any period in the last 800,000 years. This level of heat trapping gas is unprecedented in human terms — likely about as high as readings seen during the Middle Miocene 15 million years ago and at least as high as those seen during the Pliocene 3 million years ago.
Methane — another very potent greenhouse gas and the second strongest overall contributor to the climate crisis — is also continuing to rise in concentration. This rise, along with increasing CO2, has been the cause of some anxiety among scientists who monitor the global climate system.

(Rising atmospheric CO2, primarily driven by fossil fuel burning, is the main driver of the global heating crisis we are now experiencing. Image source: NOAA ESRL.)
Together with other trace heat trapping gasses, the global CO2 equivalent heat forcing is around 499 ppm during 2019 (extrapolated from NOAA data). In other words, we’ll be crossing the ominous 500 ppm CO2e threshold very soon.
What all this data means is that we have now turned the ratchet of climate crisis at least once. A set of serious impacts are now locked in. Indeed, we are seeing them. But if we keep burning fossil fuels and turn the ratchet again, it gets much worse from here on out.
(Want to help fight the climate crisis by transitioning to a clean energy vehicle? Get 1,000 free supercharger miles at this link.)
Share this:

Posted by robertscribbler on July 16, 2019
https://robertscribbler.wordpress.com/2019/07/16/what-2019s-hottest-june-ever-recorded-says-about-the-climate-crisis/
NASA: April of 2019 was Second Hottest on Record
Before we get into the latest record or near record global heat news, I’d just like to make a brief announcement. Concordant with editorial guidance from The Guardian, I’ll be changing my climate communications to more fully reflect the crisis that is now ongoing. Whenever possible, I’ll be using the words — climate crisis to replace climate change, and global heating to replace global warming.
I’ve already made liberal use of the term human forced climate change — this will change to human forced climate crisis or global heating when possible. In addition, the elevation of linkages between fossil fuel burning — which is the crisis’ primary driver — to present global heating will continue.
(Global heat for April of 2019.)
In my view, this verbiage more sufficiently communicates a necessary sense of urgency. For the climate crisis is upon us now and we are now experiencing more extreme impacts. In other words, we’ve already taken one full turn of the climate crisis ratchet by allowing fossil fuels to continue to dominate our energy systems. We don’t want to experience a second or third full turn and the related terrible tightening.
*****
The climate crisis deepens further…
According to NASA GISS, global temperatures have again jumped into near record hot ranges. Readings from this key global monitor found that April of 2019 hit 0.99 degrees Celsius above mid 20th Century ranges. This is about 1.21 C above 1880s values that bound the start of the NASA monitor. In total, it’s a value that makes April of 2019 the second hottest such month in the 139 year global climate record. And the temperatures we are experiencing now are likely the hottest annual and decadal averages in the last 120,000 years.
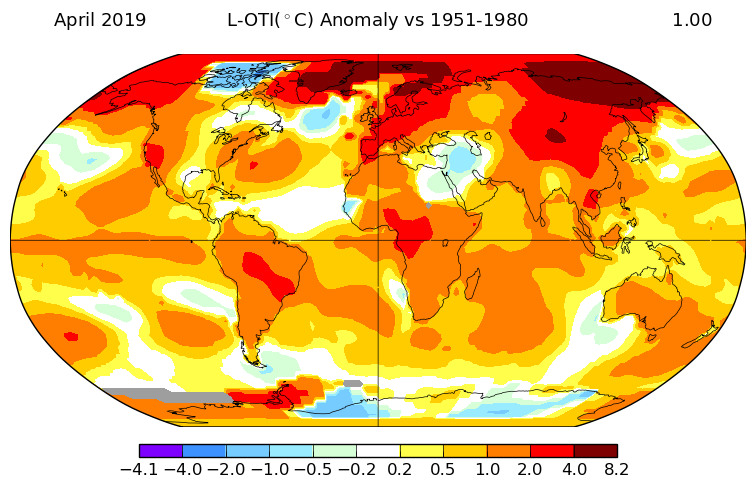
(April of 2019 anomalies paint a picture of global heat. Image source: NASA.)
Looking at the NASA temperature anomalies map above we find the greatest departures from typical April averages centering on the higher latitudes of the Northern Hemisphere. This distribution of abnormal warmth is consistent with polar amplification in which relative warming tends to center on the poles as atmospheric greenhouse gas concentrations increase. The ongoing and massive burning of fossil fuels — beginning in the 18th Century and rapidly ramping through the 20th Century — has provided the majority of these gasses. They are pushing the Earth system into the severe warming spike we now see today.
The Equatorial region also showed elevated heat — consistent with an ongoing weak El Nino (which also nudges Earth into the warm side of natural variability, making regional and global all time heat records more likely). Meanwhile, very few cool pools were found. The notable region being a persistent cool zone in the North Atlantic near melting Greenland (predicted by climate models and a facilitator of unstable weather for North America, the Northern Atlantic, and Europe).
Overall temperature track for 2019 is still behind the record hot year of 2016 (see predicted range by Dr. Gavin Schmidt above). And it appears likely that 2019 will hit in the range of 5th to 1st hottest on record. This year, however, is likely to strike close to or even above 2016 values during some months as the effect of the weak El Nino combined with the larger trend of global heating by fossil fuel burning sets the stage for potential new high temperature records.
(Want to help fight the climate crisis by transitioning to a clean energy vehicle? Get 1,000 to 5,000 free supercharger miles at this link.)
Share this:

Posted by robertscribbler on May 21, 2019
https://robertscribbler.wordpress.com/2019/05/21/nasa-april-of-2019-was-second-hottest-on-record/
Please Help Support Our Ongoing Efforts

Climate of Pandemic — A COVID-19 Special Report
GROWTH SHOCK
Luthiel’s Song: Dreams of the Ringed Vale

Luthiel’s Song: The War of Mists

Climate Progress

The Secular Jurist

Exposing Misinformation Spread by Anthony Watts

Colorado Bob’s Climate Feed

Arctic Sea Ice Blog

Science Blogs

Climate State


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}